
Primary Healthcare in South and Southeast Asia
Reading Time: 8 minutesDOWNLOADS
Executive Summary
Primary healthcare (PHC) is considered to be the bedrock of resilient, equitable, and efficient healthcare systems. Evidence suggests that a PHC system that facilitates coordinated care with integration across levels of care can improve health outcomes, enhance financial protection, and reduce burden on hospitals by emphasising prevention, early diagnosis, and community-based care. Therefore, PHC has been considered as central to achieving universal health coverage (UHC) and the Sustainable Development Goals (SDGs).
The importance of PHC has been recognised by South and Southeast Asian countries. Countries have introduced a range of policies and reforms to strengthen their primary care systems. Nonetheless, the performance of primary care varies significantly across the region. Inadequate financing, shortages of healthcare workers, fragmented governance structures, and weak coordination across levels of care are some of the challenges faced by most of the countries in the region.
This paper investigates the state of PHC in 10 countries across South and Southeast Asia: Bangladesh, India, Indonesia, Nepal, Malaysia, the Philippines, Sri Lanka, Singapore, Thailand, and Vietnam. It analyses how institutional arrangements and governance mechanisms influence PHC performance and identifies opportunities for regional collaboration. The analysis focuses on five key levers derived from the UNICEF–WHO analytical framework: political commitment, financial commitment, models of care, health workforce, and community engagement.
The paper compares experiences from these countries and highlights common challenges and approaches that can inform future reforms. The paper argues that stronger regional collaboration can help countries accelerate PHC strengthening through the sharing of knowledge, technical expertise, and institutional innovations.
Changing Health Needs in Asia
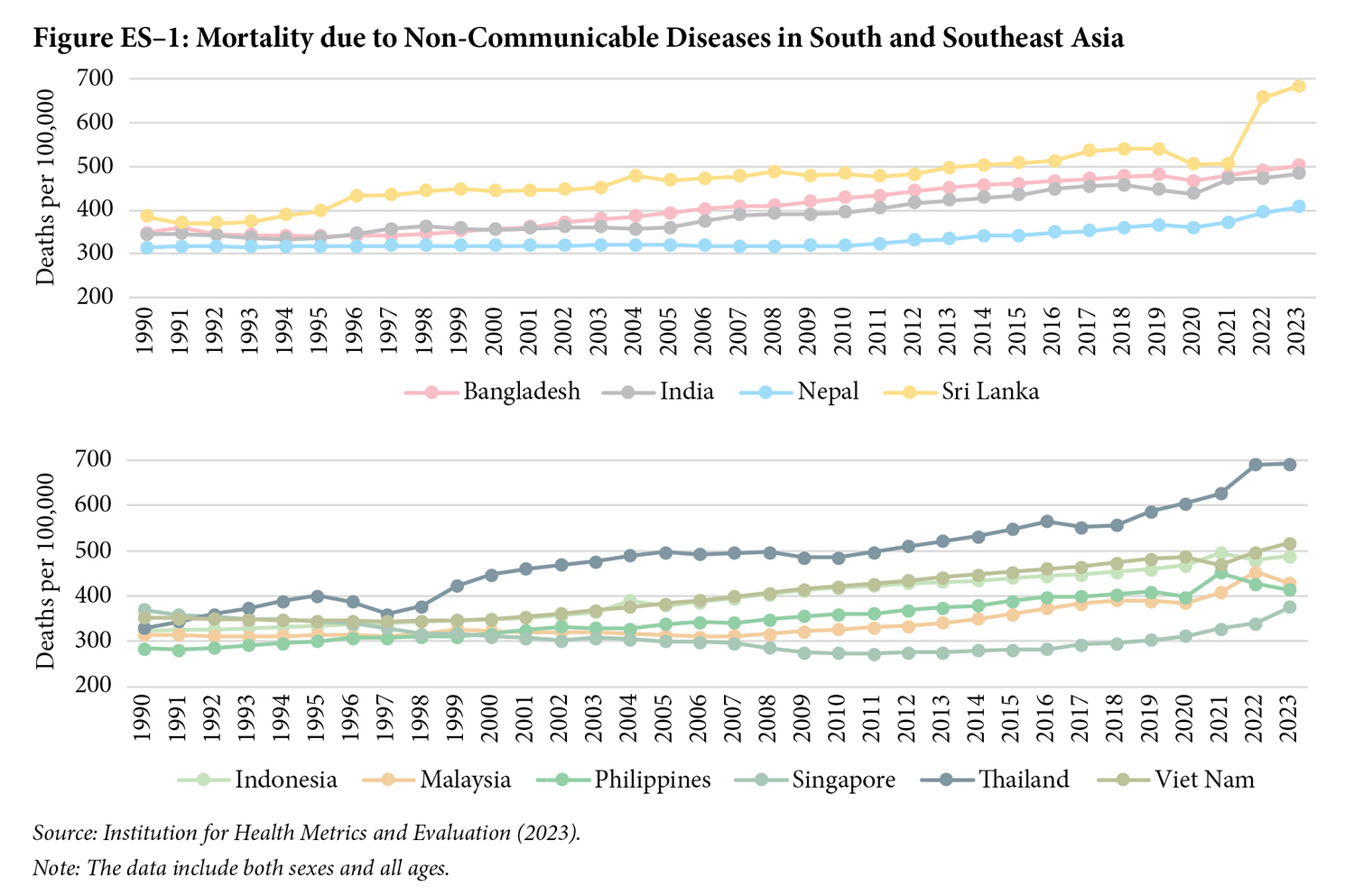
The evidence suggests that South and Southeast Asian countries are undergoing major demographic, epidemiological, and social transitions that are reshaping healthcare systems. These changes are strongly correlated with the growing number of cities. The increasing urbanisation is generating new health risks associated with lifestyle changes and environmental pollution. In addition, the proportion of elderly people is increasing, fertility rates are declining, and life expectancy at birth is increasing. All these are related to the emergence of non-communicable diseases (NCDs) such as diabetes, cardiovascular diseases, and cancers, which are becoming the dominant causes of illness and death across the region (Figure ES–1).
The literature suggests that the healthcare system needs to be capable of delivering continuous, coordinated, and preventive care in order to address the emerging needs. However, healthcare systems in the region remain heavily oriented towards hospital-based treatment rather than community-based prevention and primary care. Strengthening PHC is therefore essential to ensure that healthcare systems can respond effectively to emerging health challenges.
Political Commitment and Financing for Primary Healthcare
All 10 countries included in this study formally recognise PHC as central to achieving UHC. However, the level of political commitment and the extent of investment in PHC vary significantly across the region.
Some countries have demonstrated sustained political leadership in strengthening PHC systems. The Universal Coverage Scheme (UCS) in Thailand represents one of the most successful examples of PHC-oriented health reform in the region. Thailand has expanded access to healthcare through tax-funded financing and strong gatekeeping mechanisms, which eventually has led to reduced out-of-pocket expenditure (OPPE). A long-standing policy of free public healthcare, supported by strong preventive services and a well-developed public health workforce, has been the key characteristic of primary healthcare in Sri Lanka.
Indonesia has expanded health coverage through its national health insurance programme, Jaminan Kesehatan Nasional (JKN), which now covers a large share (~80%) of the population. On the other hand, a strong network of subsidised primary care provisioning is the key characteristic of the Malaysian primary healthcare system.
It is important to note that, despite these successes, many countries continue to face challenges in various dimensions of the PHC system. Political incentives often favour hospitals and specialised services, which are more visible and politically attractive than preventive care. As a result, PHC systems frequently remain underfunded despite strong policy commitments.
Models of Care, Workforce, and Community Engagement
The literature suggests that the organisation and model of service delivery vary across the region. Bangladesh, Nepal, Sri Lanka, and India rely heavily on public facilities and community health workers (CHWs) to deliver services at the community level. Primary healthcare systems in these countries often achieve strong outreach and community trust but face challenges related to workforce shortages and limited resources.
The mixed public–private systems, where both public and private providers play important roles in delivering primary care, define PHC systems in Thailand, Malaysia, Indonesia, Vietnam, and the Philippines. It has been found that even though the overall PHC systems often provide wider service availability, they also face governance challenges related to regulating private providers and ensuring equitable access.
Singapore represents another model in which private general practitioners (GPs) deliver a large share of first-contact services within a highly regulated system supported by strong digital infrastructure and government subsidies.
Inequity in the distribution of the workforce and overall workforce shortages remain major challenges across all these countries. Health workers are often concentrated in urban areas, leaving rural and remote communities underserved. CHWs play an important role in addressing these gaps by delivering preventive services and supporting outreach activities.
Community engagement mechanisms are also an important feature of many PHC systems in the region. Programmes such as Thailand’s Village Health Volunteers (VHVs) and India’s Accredited Social Health Activist (ASHA) illustrate how community participation can strengthen accountability and improve responsiveness of health systems.
Key Findings
Useful lessons emerged from the above discussion.
First, strong political commitment is the key to sustained public financing towards PHC systems. Second, even though countries have gone through several policy reforms, fragmentation in governance structures and institutional arrangements persists, which needs to be addressed. Third, several countries have improved workforce shortages; however, inequity in the distribution of the workforce remains. Focusing on CHWs is the key to addressing issues related to workforce shortage. Fourth, institutionalised community participation can strengthen accountability and improve trust in health systems. Finally, regional collaboration offers an important opportunity for accelerating PHC reforms through shared learning and cooperation.
Pathways for Regional Collaboration
A key argument of this paper is that South and Southeast Asian countries can accelerate progress in PHC through regional collaboration. Although countries differ in economic development and health-system design, they face many common challenges. Therefore, cross-country learning on various institutional innovations can help respective countries to design more effective reforms.
Strengthening Political Commitment and Financing
Thailand’s experience with its tax-funded UCS demonstrates how strong political leadership and sustained public financing can strengthen primary care and reduce financial barriers to healthcare. The implementation of the gatekeeping system and strategic purchasing in Thailand is a great example for countries like India, Indonesia, and the Philippines.
The national health insurance programme in Indonesia offers important lessons on expanding health coverage in large and decentralised countries. The integration of primary care services within a national insurance framework in Indonesia offers a crucial lesson for Bangladesh, India, and Nepal.
Malaysia and Sri Lanka demonstrate how long-term political commitment to publicly funded healthcare can support strong PHC systems. These experiences offer lessons for countries seeking to rebalance health spending toward preventive and community-based care.
Improving Models of Care and Governance
Coordination between primary care and hospitals has great potential in improving continuity of care. Thailand offers great insights in terms of coordinated care. The district health system in Thailand illustrates how strong coordination between primary care facilities and hospitals can improve continuity of care. India and the Philippines, which have fragmented health systems, could learn from Thailand’s experience in strengthening referral systems.
The managed care in a decentralised healthcare system in Indonesia provides a valuable lesson for India and the Philippines.
Singapore has a regulated mixed public–private primary care model. The model demonstrates how governments can maintain quality and accountability while engaging private providers. Since Malaysia, Vietnam, and India have a large private sector, they could benefit from Singapore’s regulatory approaches.
Advancing Digital Primary Healthcare Systems
The Ayushman Bharat Digital Mission (ABDM) in India aims to create a national digital health ecosystem linking electronic health records (EHRs), telemedicine platforms, and digital health identifiers. Bangladesh, Nepal, and Indonesia could learn from India’s experience in building large-scale digital health infrastructure.
Singapore’s advanced digital health systems demonstrate how integrated EHRs and strong data governance can support high-quality care. Other countries in the region could benefit from Singapore’s experience in digital health regulation and interoperability.
The SATUSEHAT platform in Indonesia illustrates how national digital platforms can integrate fragmented health data systems. Countries such as the Philippines and Vietnam could draw lessons from Indonesia’s approach to integrating digital tools with health insurance systems.
Strengthening the Primary Healthcare Workforce
India’s ASHA initiative demonstrates how CHW programmes can expand access to healthcare services in underserved communities. Countries such as Bangladesh and Nepal could learn from India’s experience in scaling and supporting CHW programmes.
The Female Community Health Volunteer (FCHV) programme in Nepal provides an example of how community-based workers can improve maternal and child health (MCH) outcomes. The VHV programme in Thailand also demonstrates how CHWs can contribute to health promotion and emergency response.
Regional collaboration could support workforce development through shared training programmes, exchange initiatives, and regional competency frameworks.
Strengthening Community Engagement
Thailand’s National Health Assembly demonstrates how inclusive governance platforms can strengthen community participation in health policymaking. Other countries in the region could explore similar mechanisms to involve citizens in health system planning.
Village Health, Sanitation, and Nutrition Committees in India offer an example of institutionalised community participation at the local level. Community Clinics (CCs) in Bangladesh demonstrate how community-based facilities can serve as accessible entry points for primary care services.
Sharing these experiences across the region can help countries design more responsive and participatory health systems.
To recap, coordinated care is the key to strengthening PHC systems in South and Southeast Asia. Governments should prioritise greater public investment in primary care and preventive services. Strong governance and regulatory frameworks are also needed to improve coordination between public and private providers. Investment in the health workforce should focus on training, retention, and the equitable distribution of health workers. Digital health systems should be strengthened to improve data integration, service coordination, and the monitoring of PHC
performance. Regional collaboration platforms should likewise be expanded to support knowledge sharing, technical cooperation, and joint learning across countries. By combining national reforms with regional cooperation, countries in South and Southeast Asia can build stronger PHC systems that are more
equitable, resilient, and responsive to the changing health needs of their populations.
Q&A with authors
What is the core message of your paper?
The paper argues that primary healthcare (PHC) is central to achieving equitable, resilient, and efficient health systems in South and Southeast Asia, but its effectiveness is shaped primarily by governance and institutional arrangements rather than policy intent alone.
While all countries recognise PHC as key to universal health coverage (UHC), implementation remains uneven due to fragmented systems, underinvestment, and weak coordination. By analysing 10 countries across five levers—political commitment, financing, models of care, workforce, and community engagement—the paper shows that how PHC is governed determines outcomes more than what reforms exist.
It further highlights that rapid demographic and epidemiological transitions, particularly the rise of non-communicable diseases, require a shift toward preventive, coordinated care.
The central contribution is a forward-looking argument: regional collaboration and cross-country learning can accelerate PHC strengthening across diverse Asian health systems.
What presents the biggest challenge?
The biggest challenge is the gap between strong policy commitment to PHC and weak implementation due to governance and political economy constraints.
Despite formal prioritisation, PHC systems remain underfunded, fragmented, and poorly coordinated. Political incentives often favour hospital-based care over preventive services, leading to persistent underinvestment in primary care. Workforce shortages—especially in rural areas—and weak regulation in mixed public–private systems further undermine service delivery.
A deeper issue is that PHC reforms yield long-term benefits and are less politically visible, reducing their appeal within electoral cycles. Additionally, PHC is sometimes perceived as a low-quality or poverty-targeted service, weakening public trust and utilisation.
These factors create a reinforcing cycle of low investment, poor quality, and continued reliance on hospitals and out-of-pocket spending, limiting progress toward equitable and efficient health systems.
What presents the biggest opportunity?
The biggest opportunity lies in regional collaboration as a mechanism to accelerate PHC strengthening through shared learning and institutional innovation.
Despite diverse contexts, countries across South and Southeast Asia face similar challenges—workforce gaps, financing constraints, governance fragmentation, and rising NCD burdens. This creates strong potential for cross-country learning.
Successful models—such as Thailand’s tax-funded UHC, Indonesia’s insurance expansion, India’s digital health systems, Singapore’s regulated PHC model, and community health worker programmes—offer transferable lessons.
Regional platforms can facilitate knowledge exchange, workforce development, digital integration, and policy coordination.
By leveraging these mechanisms, countries can move beyond isolated reforms and build more coordinated, people-centred PHC systems, making regional cooperation a key pathway for accelerating health system transformation.
Keywords: Universal Health Coverage, Health Systems Strengthening, Governance and Institutions, Primary Healthcare in Asia, Community Health Worker in Asia



Find on this page
The Centre for Social and Economic Progress (CSEP) is an independent, public policy think tank with a mandate to conduct research and analysis on critical issues facing India and the world and help shape policies that advance sustainable growth and development.