
Drivers of Primary Healthcare and Elementary Education Initiatives in Odisha (2014–2024)
Reading Time: 8 minutesDOWNLOADS
Executive Summary
Context and Research Objectives
This study examines the drivers of state-level initiatives in primary healthcare and elementary education in Odisha during 2014–2024, with a focus on urban areas and on the early stages of the policy life cycle: impetus and initiation, and conceptualisation and design.
Odisha has achieved noteworthy progress in poverty reduction and expanding access to social welfare. This is evident in improvements in maternal and child health (MCH) indicators, including infant mortality rate (IMR), maternal mortality ratio (MMR), institutional deliveries in public facilities, and child vaccinations. In elementary education, Odisha’s performance in the NAS 2021 surpassed the Indian average in several subjects. These achievements are significant given Odisha’s income disparities, fiscal history, and previously poor health and education outcomes.
Odisha is important for this study for three reasons. First, it has witnessed unusual continuity in both the political regime and bureaucracy, with some tenures spanning a decade. This makes it a useful case for asking how political stability can be an enabling factor for progressive social welfare provisioning. Scholars have commented that political leadership in Odisha has been welfare oriented. How did this stability translate into a focus on urban primary health and elementary education, which stakeholders drove policy initiatives, and which ideas did they prioritise? Second, Odisha’s financial position has improved sharply over the past two decades. It has maintained a revenue surplus since 2005–2006, and since 2015, higher non-tax revenue has strengthened domestic resources. This allows us to ask how greater fiscal space shapes social welfare provisioning and what receives attention once resources become available.
Third, the study focuses on urban areas. Although Odisha remains predominantly rural, its urbanisation is projected to increase in the coming decades (National Institute of Urban Affairs [NIUA], 2022), and more than one-fifth of its urban population is categorised as urban poor. Even if Odisha’s urbanisation remains below the Indian average, [1] the concentration of poverty, precarious living conditions, and low per capita incomes in urban areas requires greater public attention. Recent urban initiatives therefore raise an important question: How far do they address healthand education-specific challenges in urban Odisha? We examine this through the following question: Why and when did Odisha undertake state-level initiatives for primary health and elementary education in urban areas during 2014–2024?
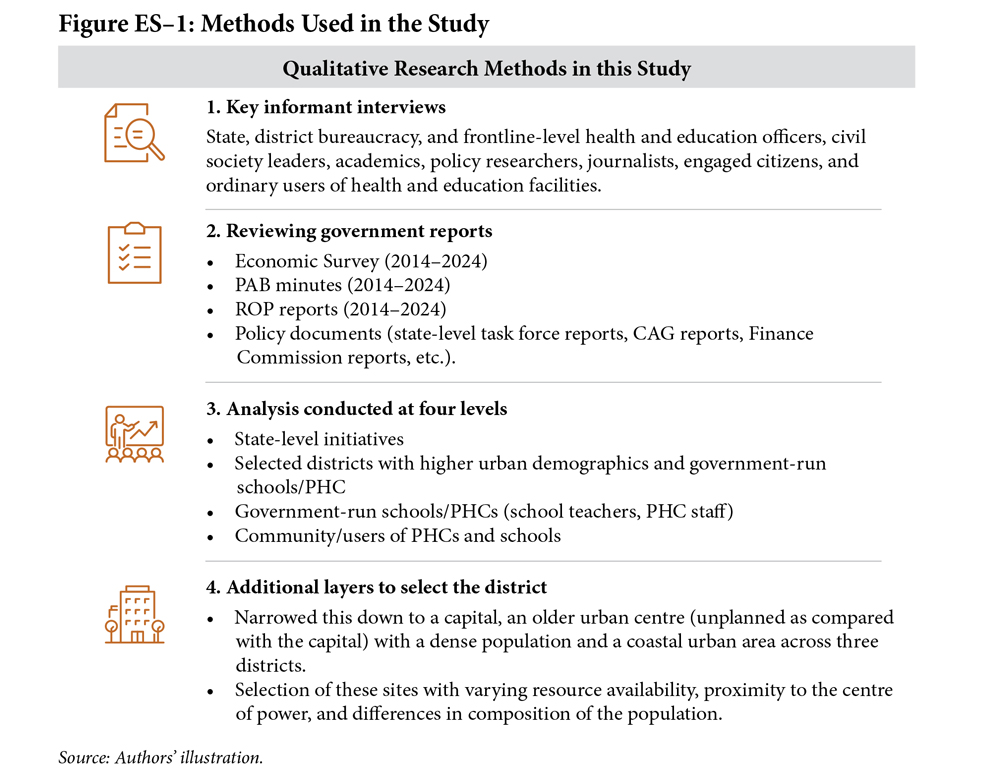
We employed qualitative methods in this study (see Figure ES–1).
Sectoral Findings and Policy Mismatches
Our study is organised in three parts. First, we examine the number and nature of initiatives. We selected initiatives that have been either funded and/or ideated by the state. We also took stock of the trends in the budget allocation to the health and education sectors during the study period. Second, we examine the objectives and the strategy of these initiatives and whether they align with the ground-level challenges faced by urban primary health centres (UPHCs) and elementary schools. Third, we examine the actors and pathways that drove state-level primary health and elementary education initiatives.
Our findings highlight that the state’s overall focus has been greater on health than on education. Within health, however, the emphasis has been stronger on tertiary care and opening hospitals than on primary care. The state’s flagship health programme during this decade was the health insurance scheme, Biju Swasthya Kalyan Yojana (BSKY). At the same time, Odisha did take note of some challenges specific to urban health, including shortages of specialists in UPHCs, public–private partnership (PPP) arrangements for staffing, and gaps in UPHC management in urban areas. Interestingly, the state has also focused on rising mental health concerns and the growing burden of non-communicable diseases (NCDs) in urban areas.
In education, the dominant focus has been on infrastructure, notably digital infrastructure under the 5T High School Transformation Programme. Major initiatives focused on alumni donations for school development through the Mo School Abhiyaan, model schools, school mergers, and free textbooks and uniforms. Elementary education received much less attention, and we identified only one clearly urban-specific initiative: the Anwesha scholarship for Scheduled Castes and Scheduled Tribes (SCs/STs) students studying in English-medium private schools in urban areas.
Our analysis of the alignment between the studied initiatives and ground realities highlights two types of mismatches: a) a problem–prioritisation mismatch, where problems that impact the uptake of UPHCs and urban elementary schools do not consistently receive adequate attention and b) a solution–challenge mismatch, where the solutions proposed by initiatives either fail to fully achieve their intended objectives or fall short of advancing the broader goal of improving uptake.
In health, despite increased budgets and policy attention, initiatives have not addressed key shortages in the health workforce and primary care infrastructure in urban areas, which manifest differently than those in rural settings. For instance, the Ama Clinic seeks to meet the demand for specialist services through weekly visits to UPHCs, but its effectiveness is limited when specialist shortages persist. Secondary studies also find that budget utilisation remains persistently low, highlighting the state’s limited spending capacity.
In education, the focus on infrastructure upgradation has not been matched by efforts to address teacher shortages or to train teachers to use digital tools effectively. Urban school governance also faces several unique constraints. Despite improvements in many health outcomes, we find reversals in some health and education indicators, including MMR, urban IMR, and government-school enrolment in Class 1. These indicate a weak capacity to sustain gains and a lack of robust monitoring systems.
Actors and Pathways in Policymaking
To understand why Odisha has focused on policy problems and the actors involved, our findings highlight the key drivers of initiatives during this decade.
First, there has been a strong central government push for major initiatives, including school mergers and UPHC extension clinics. Second, the state bureaucracy has played an engaged and dominant role. Senior bureaucrats in Odisha, led by the Chief Secretary, have shaped decision-making in health and education. With stable tenures and political support, they have had the space to select problems, design interventions, and drive implementation. At the same time, bureaucrats have faced pressure to address clearly defined problems in ways that are visible to the electorate.
The implication of this was a fractured health and education agenda, where targeted issues are addressed with limited coherence and connection. In Odisha, the prominent role of the bureaucracy in governing health and education is a consequence of a highly centralised political culture. Historically, the chief minister has been the primary political authority and the visible champion for these sectors. This dynamic, coupled with the near absence of oppositional politics (including from within the party), has created a governance model in which the focus of social welfare initiatives often prioritises generating positive public perception and political support.
During this decade, other pathways for policymaking in urban primary healthcare and elementary education, such as civil society organisations (CSOs), social movements, professional associations, and community-based organisations (CBOs), have remained muted. This is notable because Odisha has a large number of CBOs created by the government, such as active self-help groups (SHGs) and slum development committees.
Policy Recommendations
We propose four policy recommendations that can address these implications. The focus is on widening the diversity of ideas, actors, and incentives driving policy initiatives.
First, to address the limited range of initiatives in urban areas, particularly in education, we recommend creating a stakeholder-wide body at the district level. This body would identify issues and recommend amendments to existing initiatives in line with urban challenges. It would focus specifically on policy ideation for ‘urban issues’ and include all relevant stakeholders across school education and primary health: District Education/Health Officers, local CSOs, CBOs such as SHGs, donor bodies, representatives of frontline professional organisations (teachers’ unions and doctors’ unions), research professionals, activists, and select retired members of the district-level health and education bureaucracy (such as former DHOs and DEOs). These bodies should be established in all urban-dominant districts and report to a consultative panel created at the state level. Currently, alignment between top-down policy prescriptions and the ground challenges in urban areas is weak. Creating a district-level body to identify issues and suggest implementable solutions can lead to greater ownership. Given the expected increase in Odisha’s urban demographic in the coming decades, such mechanisms are needed to develop an urban agenda for health and education.
Second, we recommend creating a consultative panel at the state level that brings together the state bureaucracy and community-based CSOs, donor bodies, state-level CSOs, pan-India CSOs working in Odisha, technical assistance bodies, and consulting firms. This platform would focus on identifying key issues and focus areas, with the district-level bodies reporting to it. Such panels have previously functioned in Odisha. They were able to identify critical ground-level challenges, and several initiatives across sectors benefited from CSOs’ strong connection with the communities. Reintroducing these pathways into the policymaking ecosystem would ensure the inclusion of community perspectives in policy ideation at the state level.
Third, to address challenges in sustaining improvements across key health and education outcomes, we recommend reinvigorating third-party audits and programme monitoring as system-level checks. This body already exists within the state bureaucracy in Odisha as an entity independent of line departments, with dedicated funding and personnel. Its position within the state bureaucracy and independence from the social welfare (or spending departments) are its strengths: It allows for impartial access to government information, while also enabling an understanding of internal constraints in implementation. It can also ensure that findings from such studies reach the right audience. However, this monitoring unit has not been effectively used by welfare departments. Regular audits of government programmes and schemes in health and education are critical to highlighting the strengths and limitations of ongoing programmes, creating legitimacy on the ground for government initiatives, and mobilising stakeholders.
Lastly, to address the low engagement of elected political representatives in health and education, we recommend a biannual conference of Members of the Legislative Assembly (MLAs) focused on social welfare, including these sectors. The conference could be modelled on earlier annual conferences of state education ministers at the national level (for example, during the 1980s, the annual education ministers’ conference produced reports that shaped the 1986 National Education Policy). These events generated useful public reports that helped initiate systemic changes. Currently, political engagement in health and education remains limited. Greater formal involvement of MLAs can help highlight salient constituency-level challenges, strengthen ownership, and mobilise public awareness around issues in health and education.
Q&A with authors
What is the core message of your paper?
Odisha has had a strong revenue position since 2010, a 15+years stability of political leadership, continuity in the tenures of seniormost bureaucrats which is rare among Indian states, as well as globally recognised programs to improve the lives of urban poor. Yet, the state of primary health and education in urban areas remain below national average and on several outcomes such as Infant Mortality Rate (IMR) and learning outcomes.
There is high demand for government provided primary care among the poor and also the non-poor, those who are fast moving to low-cost (and low quality) private facilities. Odisha’s Urban Primary healthcare centres (UPHCs) and schools face critical challenges in infrastructure (eg. 39% UPHC deficit, crumbling schools facilities), staff (prominent shortages of teachers, pharmacists etc.), services (non-communicable diseases, digital education). Odisha has every advantage available to address these. But so far it has not recognised them as part of its urban development plans and policies. Without a strong Urban health and Education plan of action, Odisha’s urban economic development will remain stagnant, and over a period of time, it is in the danger of developing stark inequalities.
What presents the biggest opportunity?
Odisha’s strong revenue position and the clear focus on urban governance in tier 2 and tier 3 cities pushed by the 16th Finance Commission and 6th State Finance commission is are remarkable opportunities. 16th FC particularly provides ‘untied funds’ for Urban Local Bodies (ULBs). Furthermore, Odisha has set-up urban focused government institutions such as the Odisha Urban Academy, but they lack Human Capital focus.
Odisha needs to urgently identify and develop a set of key priorities for strengthening urban schools and UPHCs and develop consultative panels at the district and state level to build partnerships with CSOs and other development partners. Linking schools and UPHCs with ULBs for local monitoring and accountabilities can be a useful starting point, particularly for the better equipped ULBs.
Additionally, Odisha has a new government which can champion the needs of urban schools and primary care facilities as part of its distinctive contribution to Odisha’s policy ecosystem. We recommend instituting a bi-annual conference of MLAs to ensure a systematic pathway through which MLAs can also idea and support health and education in their constituencies.
What presents the biggest challenge?
As a primarily rural state, which is yet to solve the crippling challenges in tribal and remote areas and improve the position of some of the most vulnerable communities in India, it is hard to convince the government to focus on urban problems. Private players fill in the gaps and generally, building facilities and providing staff is not as challenging.
Additionally, urban governance is weak even in the most urbanised of states such as Karnataka and the shortfalls facing Odisha’s ULBs in finances, functionaries, capacity and technical know-now, are even deeper. Odisha’s 6th State Finance Commission also recognises these challenges in its final report. Without effective local governance, it is difficult to improve schools and UPHCs. Rural primary care facilities and schools benefit from local monitoring and oversight.
However, the role of policy thinking is to take future oriented actions, which Odisha has done in many important areas. It must also take advantage of its unique revenue position and lay the groundwork for dedicated financing for urban health and education in the coming decades, which is needed to build a skilled, healthy population in urban centres.
FOOTNOTES
[1] SBI’s Research Report, ‘Precursor to Census 2024’ projects a 19% urbanisation rate for Odisha in 2024, which is lower than India’s projected average urbanisation rate of 35.4%.
Priyadarshini Singh
Anoushka Gupta



Find on this page
The Centre for Social and Economic Progress (CSEP) is an independent, public policy think tank with a mandate to conduct research and analysis on critical issues facing India and the world and help shape policies that advance sustainable growth and development.