
India’s Health Status and Emerging Priorities
Reading Time: 18 minutesDOWNLOADS
The recently released National Family Health Survey (NFHS 5) data presents some good and some sober news. Combined with the latest National Health Accounts (for 2017-18), also recently released, this paper attempts to outline some of the emerging priorities for health policy in India.
That there has been progress between 2014-15 and 2019-2020 on multiple health indicators is evident from the data released. The most prominent area of progress has been on Total Fertility Rate (TFR), which now stands at 2.0; below the replacement level of 2.1. While state differentials continue to exist, most states have made progress and the country as a whole is doing well on containing population. What this also suggests is the implications for women, who will be able to better manage their own and their children’s health, and as a family invest more on education for their children.
Declines in most mortality indicators – neonatal mortality rate (NMR), infant mortality rate (IMR) and under five mortality rate (U5MR)– point to better coverage of health interventions, and a better performing health system. Improved coverage is also evident from data on immunisation, Ante Natal Care (ANC) coverage, institutional deliveries, and other process indicators, all of which would have contributed to improve mortality outcomes.
The progress on nutrition, while present, is marginal, with a very small increase in the proportion of severely wasted children.
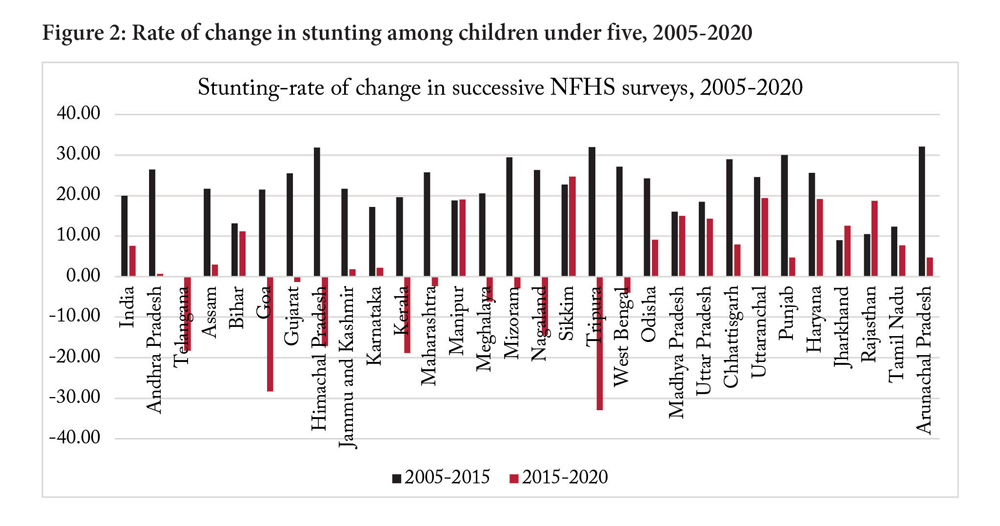
The progress on nutrition, while present, is marginal, with a very small increase in the proportion of severely wasted children. India has struggled with high levels of stunting, and this has reduced from 38.4 to 35.5. Progress in stunting is seen in the less developed states, largely in north and east India, including Bihar, UP, Rajasthan, Jharkhand, MP, Orissa. Some of the southern and western states have fared worse on stunting such as Maharashtra, Gujarat, Kerala and Telangana.
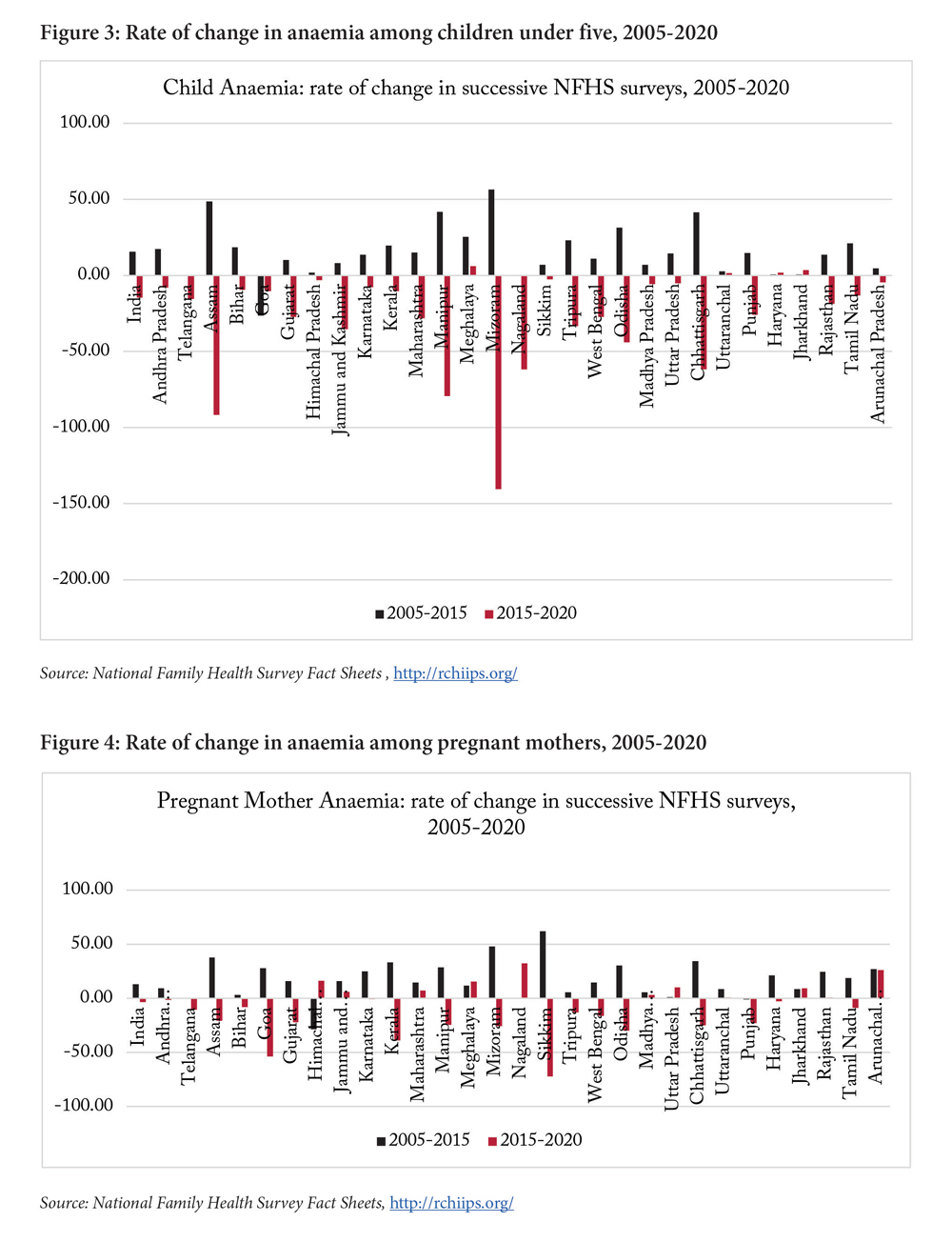
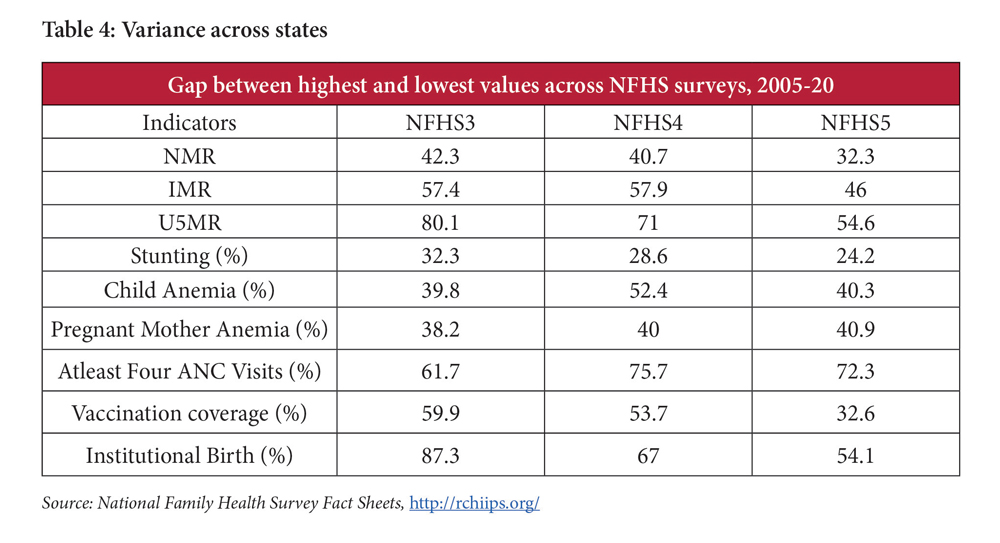
On the sober side, the country continues to fare poorly on several nutrition indicators with increasing incidence of overweight children and rising anaemia amongst children and women. A worsening status since the last round of the survey in 2014-15 is highlighted by the increase in the proportion of anemic children from 58.6 to 67.1 percent, in pregnant mothers from 50.4 to 52.2 percent, and amongst all women of reproductive age from 53.1 to 57 percent.
Non communicable diseases have increased, with higher levels of blood sugar incidence and hypertension.
On the process front, while institutional deliveries have increased, the proportion of caesarean section births have also increased. Coverage on four ANCs shows an increase of about 13 percentage points in the 2015-2020 period, and immunisation levels 23 percentage points.
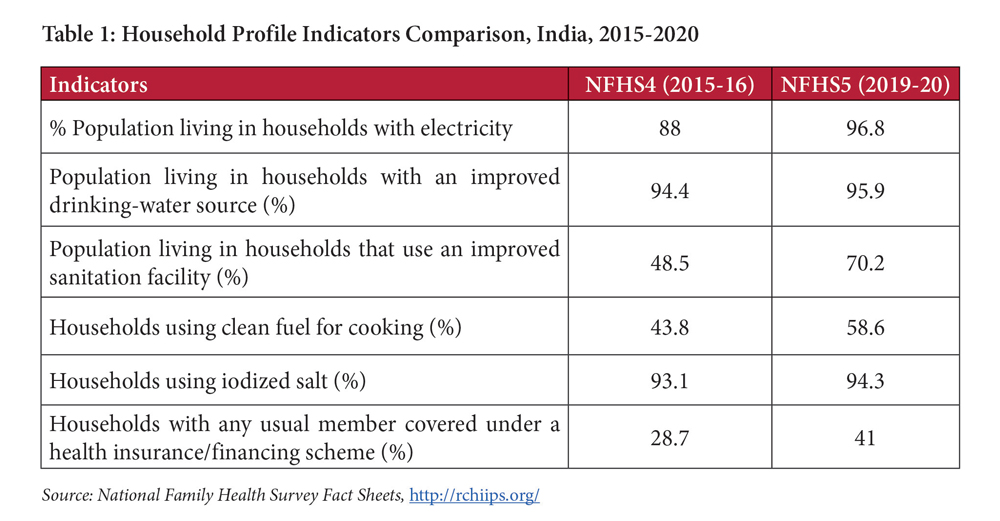
Beyond health, coverage indicators for basic needs such as electricity, drinking water source, sanitation, clean cooking fuel have all improved, though some marginally, all of which have implications for health status. Some of these improvements point to the success of national programs such as Swachh Bharat Abhiyan aimed at sanitation and Ujjwala Yojana aimed at clean cooking fuel through LPG.
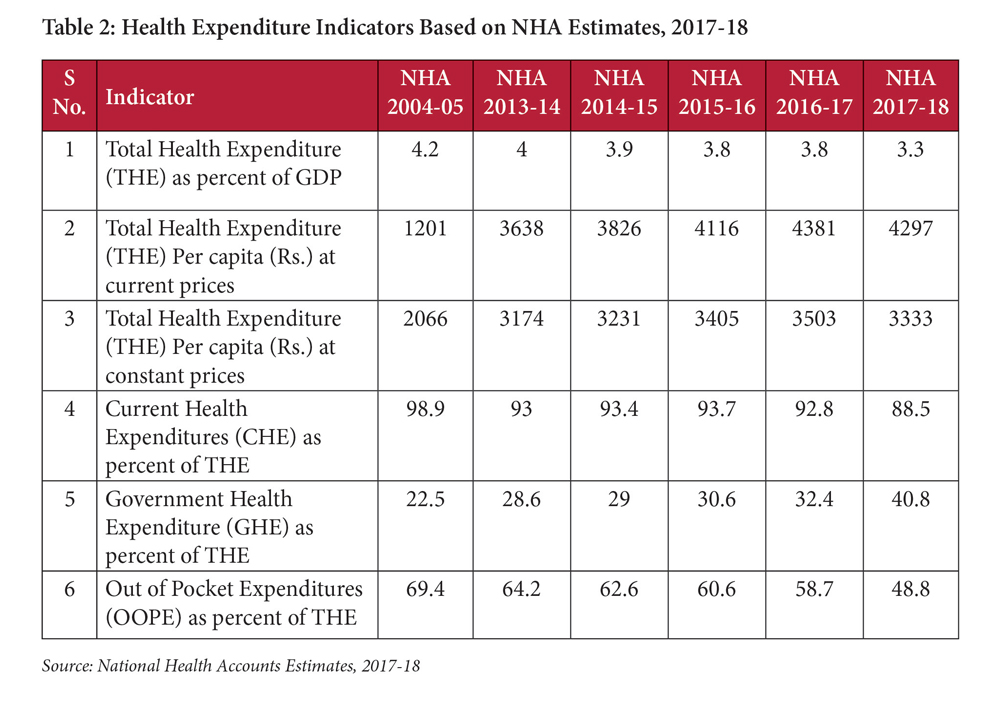
An analysis of expenditure on health, per the National health Accounts 2017-18, reveals an increase in government health expenditure (GHE) and a consequent reduction in out of pocket expenses on health (OOPs). Some scholars have argued however, that the reduction in OOP is due to forgone care, resulting from distress1. A reduction in unmet need could well account for the reduction in total health expenditure.
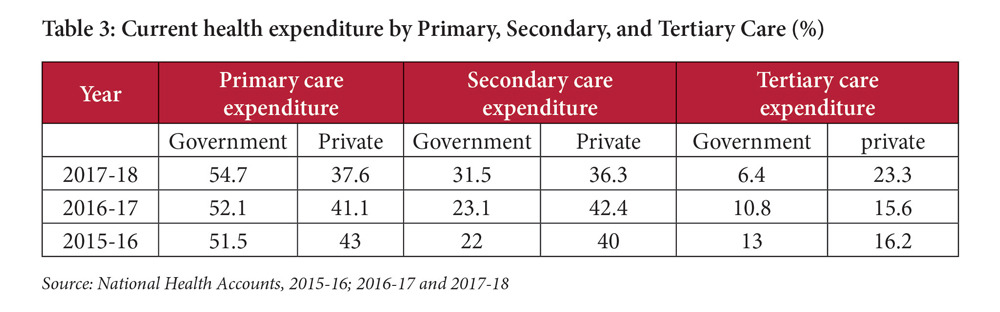
Of total government health expenditure, 54.7 percent is directed at primary care, 31.5 percent at secondary care and 6.4 percent at tertiary care. The respective figures for private providers is 37.6 percent, 36.3 percent and 23.3 percent. Compared with previous years, while there is an increase in government primary care expenditure, it is not significant.
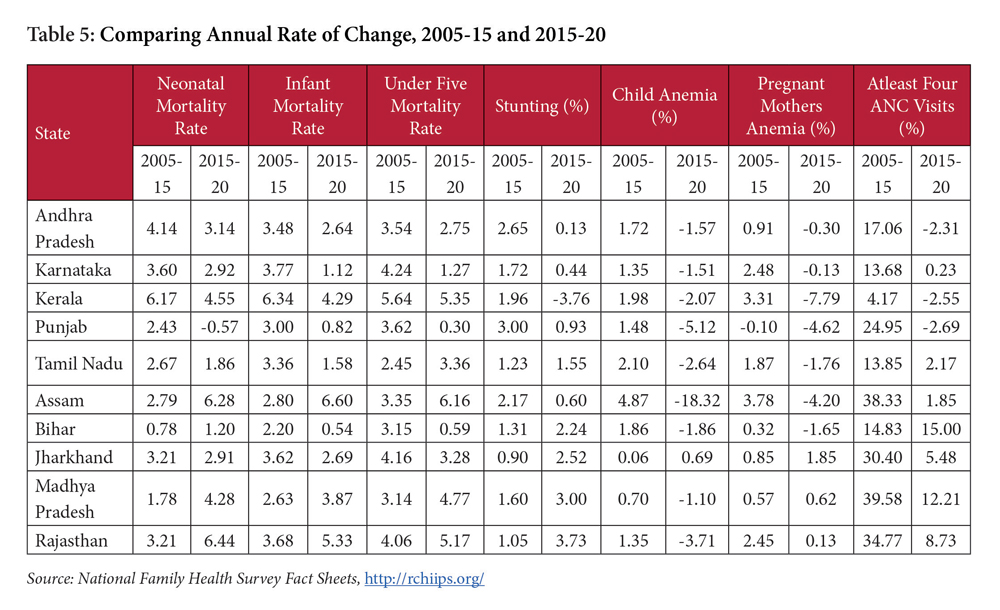
Alongside acknowledging improvements in the health status, a disaggregated analysis suggests emerging policy priorities going forward. The analysis below is based on the data currently available, which does not include disaggregation by urban/rural, gender or income level. On the availability of disaggregated details, a deeper analysis will be possible. This section compares change across two survey periods: 2005-2015 and 2015-2020. While we recognise that they are not the same duration, comments on the change account for the 10 year versus five year period, with the caveat that change does not necessarily have to be linear.
Mortality Declines
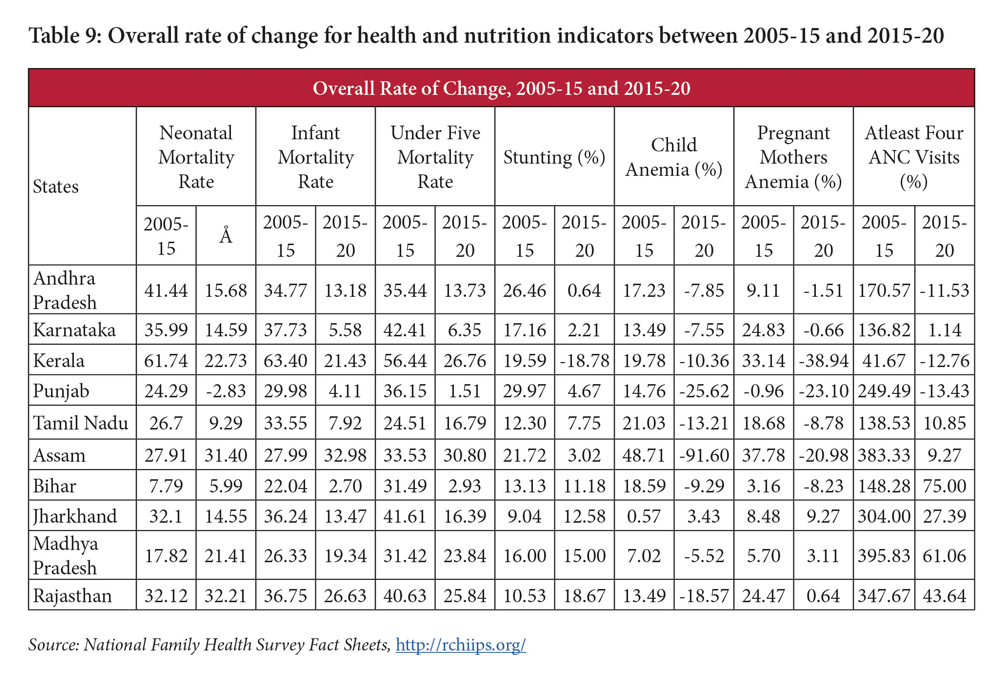
While Neonatal Mortality Rate (NMR), Infant Mortality Rate (IMR) and Under 5 Mortality Rate (U5MR) have all declined, the rate of decline has slowed: the change for NMR across NFHS 4 and 5 (2015-2020) is one third or less of the change across NFHS 3 and 4 (2005-2015) for states with the highest NMR (Kerala, Tripura and Arunachal Pradesh). Having the change in the 2005-2015 period for ease of comparison with 2015-2020 period also points to a slower decline in the later period. IMR declines show a similar trend, with multiple states witnessing a sharp decline in the rate of improvement between the two period: a 94 percent drop for Maharashtra, 66 percent for Kerala, 76 percent for Tamil Nadu. The trend is the same for most of the less developed northern and eastern states, with the exception of Uttar Pradesh which shows an increase in the rate of change (across NMR, IMR and U5MR). The data reveal similar overall trends for U5MR.
Even though many developing states such as Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, have shown signs of improvement in child nutrition but in absolute terms, they are far behind states such as Kerala and Tamil Nadu.
Though mortality rates have declined in the successive NFHS surveys, India continues to be behind in terms of achieving targets set in the National Health Policy 2017 (NHP 2017). The policy set IMR, NMR, and U5MR targets at 28 by 2019, 16 by 2025, and 23 by 2025; the current status being 35.4, 24.9, and 41.9, respectively. The status of mortality rates at the state level reveals high variations. Data reveal vast differences across states from mean value of mortality rates: NMR (mean- 19, high (25+) for seven states, low (15-) for eight states), IMR (mean-28, high (above 35) for eight states, low (below 15) for four states), U5MR(mean-33, high(above 40) for eight states, low (below 20) for five states. The significant differences in the mortality rates across states, such as Kerala (NMR 3.4, IMR 4.4, and U5MR 5.4), and Bihar (NMR 34.5, IMR 46.8, U5MR 56.8), poses questions on the implementation of child related health and nutrition programmes, especially in terms of reducing gaps between states. Existing evidence has pointed to the criticality of the first 1000 days for children to survive and thrive, with food and nutrition being immediate drivers of child malnourishment, contributing to mortality. The NFHS 5 data suggests that the percentage of severely acute malnourishment has increased in many states including Andhra Pradesh, Telangana, Assam, Gujarat, and Maharashtra. Even though many developing states such as Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, have shown signs of improvement in child nutrition but in absolute terms, they are far behind states such as Kerala and Tamil Nadu.
Maternal Health
While increase in institutional births indicates successful implementation of cash transfer incentives through Janani Suraksha Yojana and other state specific programmes related to deliveries, it is observed that birth due to caesarean has also increased simultaneously. While the national average has witnessed an increase of 25 percent of caesarean births over NFHS 4 data, states such as Tamil Nadu witnessed a 32 percent increase, Orissa 56 percent. The increase in public facilities is higher, at 20 percent, although at 14 percent caesarean sections currently, that remains within the medical norms. Caesarean births in private facilities, at 47 percent are extraordinarily high, pointing to the need for greater regulation of maternal deliveries. Moreover, despite deliveries being covered within insurance schemes, out of pocket expenses (though reduced) remain.
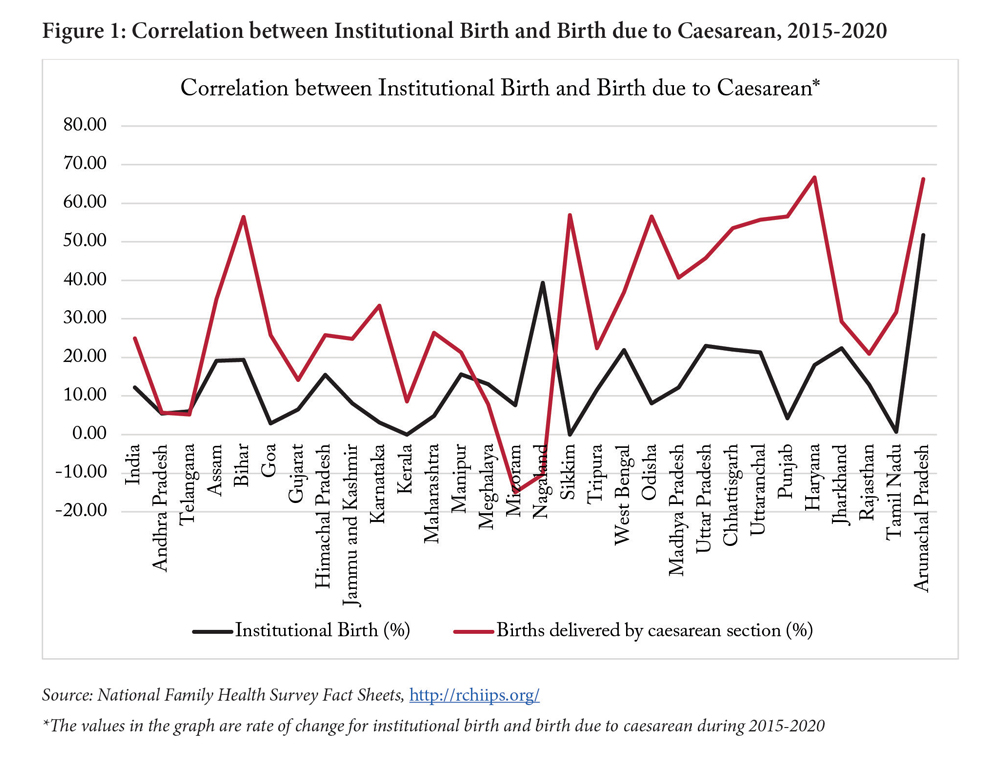
Even though WHO guidelines related to deliveries suggest that birth due to caesarean (for medical reasons) should typically be in the range of 15%, many states such as Kerala, Tamil Nadu, Telangana, Andhra Pradesh etc., had already crossed this limit in 2015 (NFHS4 data). NFHS5 data now suggests that rate of birth due to caesarean sections is increasing at a significant rate in the developing states as well. The rate of change is above 50% in Bihar, Uttaranchal, Chhattisgarh, and Odisha. Existing research has suggest a correlation between birth due to caesarean and maternal and child mortality (Leonard, Main, & Carmichael, 2019). The increasing rate of caesarean deliveries in developing states could be a cause for concern for maternal and child mortality, which is already high in these states (as per sample registration system data 2016-18, average Maternal Mortality Rate of developing states is 161). It has also been found that children who are born due to caesarean are more likely to be obese and vulnerable to respiratory infection (Temmerman & Mohiddin, 2021). Given the fact that the percentage of overweight children has also increased during the same period (2015-2020), how far the increase in overweight children is related to caesarean births will be an important question for inquiry.
Progress on ANCs and immunisation in the 2015-2020 period is significantly slower than the period of 2005-2015, where ANC cover improved 241 percentage points and immunisation cover 42 percentage points in the 2005-2015 period as compared with 13 and 23 percentage in the latter period. At current cover of 51 and 76 percent respectively, these remain low. Importantly, variations in ANC coverage across states are wide: Goa, Tamil Nadu, and Jammu and Kashmir registered more than 80 percent ANC coverage whereas Bihar (25.2%), and Nagaland (20.7%), have less than 30 percent coverage. The good news is that improvements in the ANC coverage during 2015-2020 period are relatively greater across the less developed states such as Bihar, UP, Uttaranchal, MP, Rajasthan. Immunisation coverage has declined, though very marginally, in Kerala, Goa, Sikkim and Punjab, but improved in most states. The status in vaccination coverage is different where states such as Kerala, Punjab, Haryana, Gujarat, and Maharashtra, have not performed well, registering less than 80% coverage, and EAG states such as Odisha, Rajasthan, and Uttaranchal, have registered more than 80% vaccination of children under five.
Nutrition
Improvements in stunting have been noted by the survey, with two aspects that stand out. One, stunting levels have largely improved amongst the less developed states such as Bihar, UP, Jharkhand, Madhya Pradesh, Rajasthan, but increased in some of the more developed states such as Kerala, Telangana, suggesting a trend of ‘catching up’ by the former states. Two, the rate of decrease between the 2005-2015 and 2015-2020 period suggest a slowing down of progress. While the improvement in the first period was 20 percentage points, the second period saw an improvement of merely 7.5 percentage. Adjusting for the differences in the duration of the two periods, 10 years versus five years, the 7.5 percentage is still lower than the adjusted 10 percentage points for the earlier period. Rajasthan is amongst the few states that shows an improvement in the 2015-2020 period over the 2005-2015 one.
Improvements in anaemia amongst children were noted in the 2005-2015 period, with some states demonstrating as much as 20 percent improvement. The 2015-2020 period shows a complete reversal on this front, with most states showing a deterioration in anaemia levels; with change being minimal in the states that did not worsen. In the case of anaemia levels for pregnant women, 18 states saw a deterioration in the 2015-2020 period (including states such as Tamil Nadu, Kerala, Telangana, Gujarat, Orissa, Chhattisgarh)2; seven states saw an improvement of two percentage points or more (Himachal Pradesh, Maharashtra, Meghalaya, Nagaland, Uttar Pradesh, Jharkhand, and Arunachal Pradesh) and the remaining were largely the same. In the case of anaemia for all women, Kerala shows an approximate five percentage point decline through the 2005-2020 period.
The worsening of anaemia levels is a critical issue for India, for health, productivity and income and its inter-generational impact highlights implications well beyond the individual.
The worsening of anaemia levels is a critical issue for India, for health, productivity and income and its inter-generational impact highlights implications well beyond the individual. Existing evidence suggests that women entering into pregnancy with anaemia has a negative impact on fetal growth, birth weight of the child, and maternal health. This is one of the underlying causes of child undernutrition. Recognising the intergenerational aspect of malnutrition, and the need for multisectoral intervention, the government conceptualised and launched the National Nutrition Mission or POSHAN Abhiyaan. However, the NFHS5 data poses questions on the effectiveness of the program.
The policy intervention for addressing anaemia has, in large part, been in the form of iron and folic acid (IFA) for pregnant women. While NFHS 5 shows an increase in the IFA intake for 180 days, this remains low at 26 percent. The question at the policy level is whether IFA consumption during pregnancy, even if it were to increase, is adequate for addressing anaemia, given that a couple of months of the pregnancy period would be lost by the time a woman discovers she is pregnant. Addressing anaemia requires interventions that start during childhood, continuing into adolescence, and there are few focused interventions in that regard.
Anaemia levels and extent of overweight children both point to challenges with diet, although of different kinds. The proportion of children age 6-23 months receiving an adequate diet stands at 11.3 percent, a small increase from 9.6 percent in 2015. The systemic response has continued to focus on food security, which while critical, is targeted at calorie intake rather than nutrition security. Despite debates on the need for reviewing both the Public Distribution System and meal programs (ICDS and school), the nutrition value within food programs remains a challenge. An increase of overweight children points to new risks, including an increase in NCDs.
Analysing the variance across states (highest performer versus the lowest perform) reveals a decreasing gap for most aspects except anaemia and ANC coverage (Table 4) and a disaggregated analysis of progress reveals a declining rate of change across years for some states (Table 5). For mortality and stunting indicators, states with high socio demographic status had comparatively greater annual rate of change during the period 2005-15, but the EAG states have improved during the 2015-20 period. This points to convergence between these sets of states for these indicators. Anemia shows poor performance across states. For ANC visits, though EAG states have done better comparatively, their rate of change decelerated during 2015-20, except for Bihar. There is thus a convergence visible with respect to mortality, stunting, vaccination, and institutional births, but not prominent in ANC.
Non Communicable Diseases
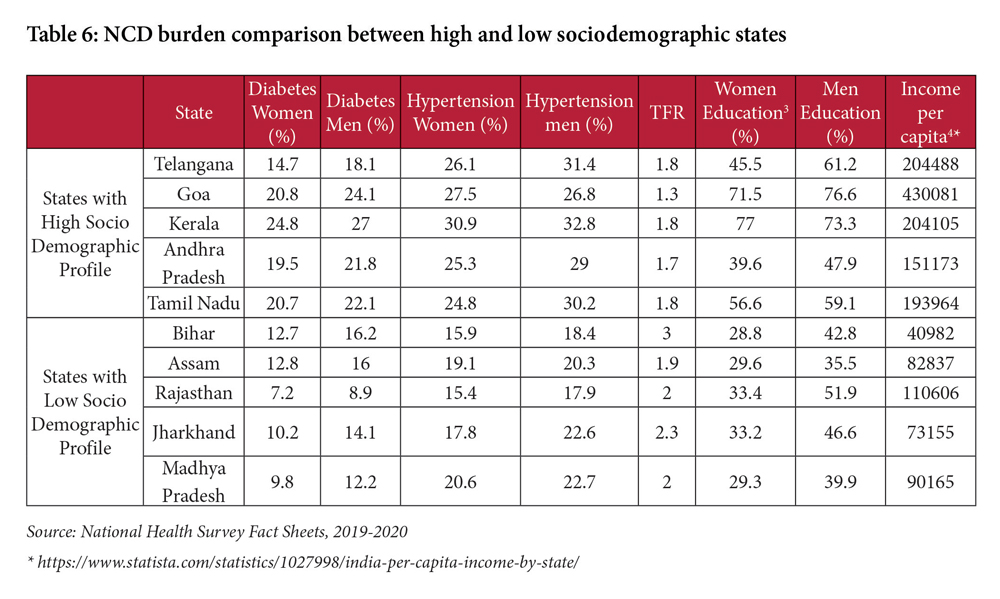
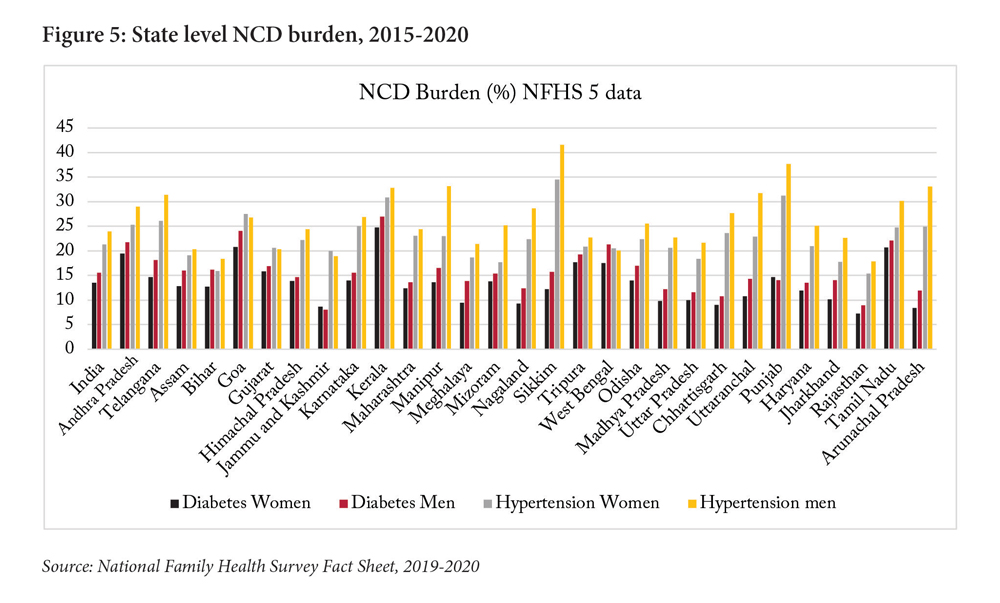
Higher sugar levels are visible in states such as Kerala, Tamil Nadu, Andhra Pradesh; and higher hypertension levels in TN, Kerala, AP, Karnataka, Maharashtra, Telangana. The Non communicable diseases (NCD) data presented in Figure 5 show that all states have gone through an epidemiological transition where states like Kerala, Tamil Nadu, Karnataka, Goa, Punjab, Andhra Pradesh, and Telangana have comparatively higher percentage of NCD cases such as hypertension and diabetes, whereas Bihar, Rajasthan, Assam, Uttar Pradesh, and Madhya Pradesh (the developing states) have lower proportion of hypertension and diabetes. The data suggest that states with higher social and demographic profile i.e., lower TFR (below replacement level 2), higher average year of education (more than 50 percent of women attending 10 or more year of schooling), and higher income per capita (see Table 4 and Lancet, 2017 and IHME, 2021), also have a higher NCD burden. The data also show that the proportion of deaths due to NCD in these states have crossed more than 70% (Kerala 81%, Goa 79.26%, Tamil Nadu 72.4%, Punjab 75.55%), suggesting that NCD management through the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular disease and Stroke, will demand greater resource allocation than communicable diseases which now comprise 15-19% of the total burden of disease. As the potential causal factors for NCD lie somewhere in the rapid unplanned urbanisation, globalisation of unhealthy lifestyle, and population aging, it becomes crucial for states with high NCD burden to devise a comprehensive policy approach focusing on intersectoral collaboration to reduce modifiable risk behaviours associated with various types of NCDs. Besides this, these states will need to invest more in management of NCDs which includes detection, screening, and treatment, and providing palliative care for people in need, pointing to the need for stronger primary care systems.
Gender
There is a notable improvement in the sex ratio, but some have pointed to possible measurement errors that may have occurred due to migration. Leaving that debate aside, the data reveal an improvement in early marriage for girls, from 26.8 percent to 23.8 percent. While indeed an improvement, the reduction is low and the extent of early marriages remains high, which is critical from the perspective of disruption in education, early child bearing and its impact on women’s and the child’s health (in particular nutrition levels). Continued attention and stronger policy interventions are required to reduce this further.
As mentioned, the reduction in TFR bodes well for population stabilisation and for women’s and children’s health. To be noted however is that the burden of family planning continues to be on women, with female sterilisation being the highest form of contraception. While the health system offers men’s sterilisation, its uptake remains stagnant and extremely low at 0.3 percent. Much more by way of communication and other forms of incentives are needed to balance the burden of contraception across women and men.
Violence is a key aspect impacting women’s health status and their ability to access healthcare. Ever-married women age 18-49 years who have experienced spousal violence, though reduced since the last survey, remains high at almost 30 percent. Another area of attention points to reviewing the extent to which India’s health system is geared to respond to this context, through designing programs and training health workers to incorporate this reality.
Health Expenditure
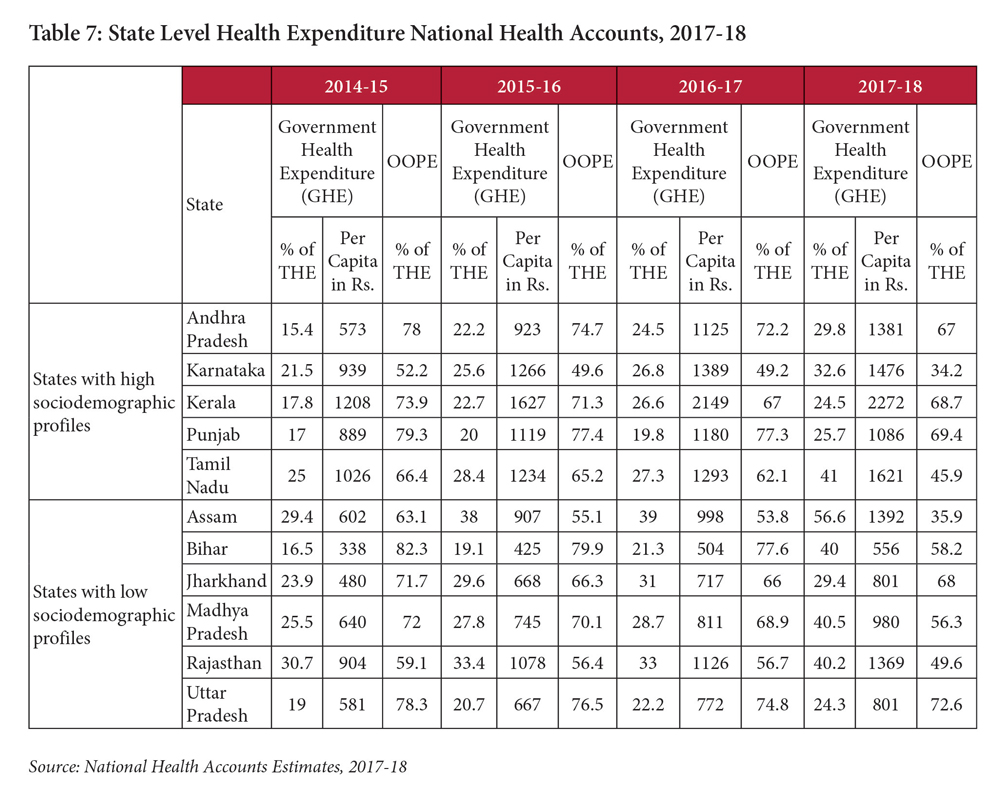
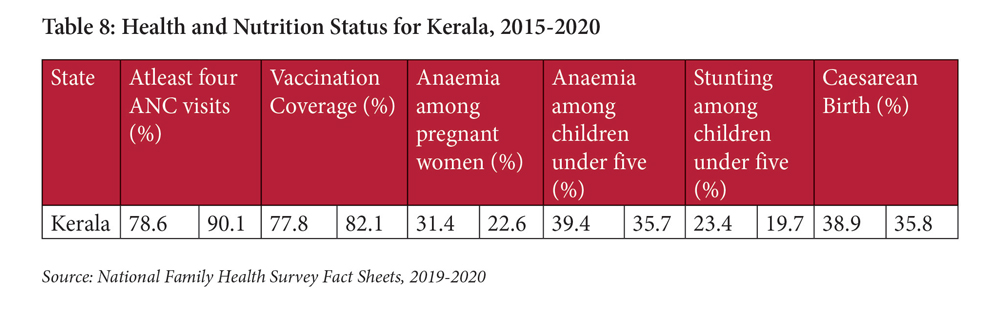
Expenditure data from the National Health Accounts reveals that most states have consistently increased the percentage of government health expenditure (GHE) in total health expenditure (THE). Increasing GHE suggests lower out-of-pocket expenses, which in turn point to the potential for better utilisation of funds directed at health. Where states have high proportion of health expenditures as a proportion of total state expenditure (GGE), but a low GHE:THE ratio, OOPs have been high, with possible inefficiencies in spending. Kerala, as an example, spends more than seven percent of its total state budget on health, yet has high OOPs at almost 69 percent, with GHE at less than 25 percent of THE. Such an architecture could be responsible for Kerala having high caesarean section births at 38.9 percent. Himachal Pradesh, on the other hand, also spends above seven percent of total state spend on health, but with a GHE at a high 48.6 percent, and a caesarean section birth rate of 21 percent.
There has been significant increase in government expenditure on health as percentage of total health expenditure across all the states, especially Bihar and Assam where the expenditure increased with the rate of 142 percent and 92 percent respectively, which is also reflected in reduction in the out-of-pocket expenditure. However, EAG states spend more in terms of GHE as percentage of THE, which is intriguing because increase in public health expenditure is not commensurate with the improvement in outcome indicators except child mortality.
The progress on several indicators since the 2014-15 survey points to the success of interventions on various fronts, although a cross-year comparison reveals that progress has slowed down for many states.
The progress on several indicators since the 2014-15 survey points to the success of interventions on various fronts, although a cross-year comparison reveals that progress has slowed down for many states. The gap between states has narrowed on most indicators between the period 2005 and 2020, pointing to a convergence between states, though not consistent across all indicators. Mortality and stunting indicators showing a decline in the rate of change for states having high socio demographic status, but an improvement in the rate of change for EAG states shows a convergence across EAG and non EAG states on several fronts. An improvement in the rate of change for EAG states, despite lower expenditure in comparison with non EAG ones, points to the need to examine the efficiencies of expenditure in non EAG states.
The NFHS5 data poses several questions on maternal and child health related programs at various levels. Women and child nutrition status has worsened in terms of deteriorating anaemia rate both at state and national level, and there is increasing inequality between developing states and better developed ones. The UNICEF framework on malnourishment suggest that maternal health is one of the underlying factors behind child undernutrition and mortality. Accordingly, the government introduced programs aimed at ante natal care services to curb cases of anaemia and child undernutrition. However, with average ANC coverage at 58 percent, and with considerable inter-state variations ranging from 80 percent to less than 30 percent, these need a review.
The other aspect of malnutrition points to food programs, which are in large part aimed at food security and need an equal focus on nutrition security. The response to nutrition needs to be more holistic, taking into account its links with mothers’ education (women with 10 or more years of schooling is 41 percent), clean drinking water, and sanitation.
Improvements in nutrition, and related improvements in maternal health need a strong primary health care system. High levels of sugar/diabetes, hypertension further underline the same need. With a reducing TFR, India’s population will become older, as has been noted by many. This will imply new health risks and a different burden on, and needs from, the health system. Much greater attention will need to be paid to conditions other than maternal and child health and infectious diseases, which forms the predominant part of the current health system focus. Admittedly, there is recognition of the need to address the growing burden of NCDs, through the Health and Wellness Centres but funds for a strong primary care system that can prevent and manage these will need more attention.
The National Health Policy (2017) had recommended that 67 percent of the total health expenditure be directed to primary care, with the 15th Finance Commission recommended the same. Yet, this currently stands at 47 percent (both public and private) and 55 percent of government expenditure. The need for increased investments to primary care, and focus on greater attention to more effective primary care are underlined by the latest health status.
For states such as Kerala, Tamil Nadu, Andhra Pradesh, Karnataka, Maharashtra and Telangana, this needs particular attention. These are also the states where anaemia levels amongst children have increased since the last NFHS survey and increased or remained stagnant amongst pregnant women. ANC visits in most of these states, notably Kerala, Andhra Pradesh, Telengana, have decreased since the last survey, while largely remaining the same in Karnataka and Maharashtra, but increasing in Tamil Nadu by about 11 percent. Vaccination coverage has seen an increase in the period between 2015-2020, but the rate of growth in the period is lower than the 2005-2015 period. Kerala is the only state that saw a decline, though nominal, in vaccination coverage. It will be important to interrogate why states like Kerala have not matched their previous performance, and whether allocative inefficiencies in health financing have led to funds not being directed in the most optimal manner.
Most of these aspects are a function of primary care. States where progress has been stagnant or has deteriorated need urgent attention in this area. These are also the states amongst the highest caesarean section births, which points to a large focus on secondary/tertiary care. It is possible that the increasing attention to insurance schemes (visible across several states) has emerged at the cost of the neglect of the primary care system, with these schemes covering only secondary and tertiary care.
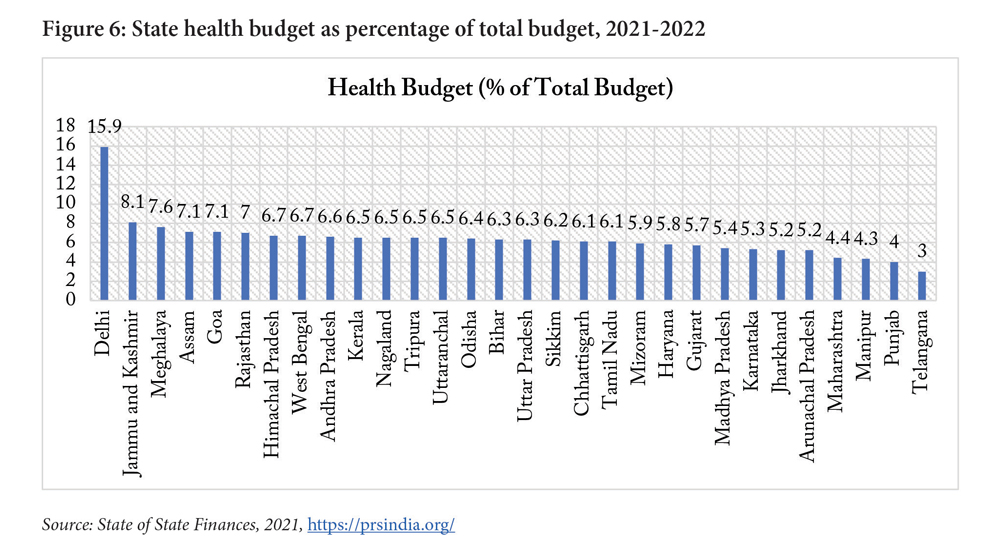
Not only is the focus on primary care an issue that needs attention, but allocation to health across states needs attention. Despite the recommendation of the National Health Policy, 2017 and its reiteration by the 15th Finance Commission, that states allocate eight percent of their total budget to health, this has averaged six percent (Figure 6).
The most sobering aspect of the health status has been on nutrition. Analysing the allocations to nutrition therefore, a study by the Centre for Policy Research found that allocations for the Supplementary Nutrition Program (2019-20) were 44 percent of the required resources calculated by them3. The cross-state analysis revealed that allocations as percentage of required cost were less than the national average for Kerala (30 percent), Maharashtra (39 percent), and Telangana (42 percent).
The data unambiguously underlines an important fact that the context and needs across states are variable, even though a standard program is implemented across the country. Kerala, for example, has a high level of institutional deliveries, but poor outcomes in anaemia and NCDs. Yet, the allocations for the program that incentivises institutional deliveries (Janani Suraksha Yojana) continues per norms that do not take into account the ground reality and result in approved budgets for this program being 183 times the required resources (Kapur et al, 2020). That this may be at the cost of other potential areas of attention, such as anaemia, ANCs and vaccination coverage, needs attention through the exploration of more flexible funding, and the state’s own design of health financing.
While disaggregated data across social and other identities is not yet available, the data on gender suggests the need for a health system much more focused on aspects of gender and its interaction with health access and outcomes. Early marriage and violence against women are not merely social issues, but key drivers of women’s own and their children’s health status. Early marriage is an important variable for women’s nutrition, and consequently, the child’s nutrition. All of this suggests the need for a stronger convergence between the ministries of health and women and a deeper gendered approach to health delivery.
In an effort to reduce TFR, several states have deployed discriminatory policies in terms of postings, official positions and other aspects, linked with the number of children. Even though these have been debated extensively, they have continued, despite the implications for deepening discrimination against women and increasing foeticide. With TFR levels improving, there is an urgent need to review such policies.
The latest health status dataset in the form of NFHS 5 presents some good and some sobering news. There is progress on most fronts, though not very significant on several, and a deterioration on a few aspects. Importantly, it is the inter-state variations, with very variable shifts across indicators, that point to where attention is needed. There are at least four key implications emerging, or reinforced, from the recently released data sets. One, the need for greater fiscal flexibility to states to enable innovation and contextually relevant interventions that respond to the specific needs of the state. Two, increased expenditure on and attention to primary care. Three, an increased allocation by the states to health. Four, a gendered approach to health delivery.
Kapur, A., Shukla, R., Thakkar, M. & Menon, P. (2020). Financing Nutrition in India: Cost implications of the new nutrition policy landscape, 2019-20. Accountability Initiative. New Delhi: Centre for Policy Research and International Food Policy Research Institute. https://accountabilityindia.in/wp-content/uploads/2020/07/Financing-Nutrition-in-India-AI-IFPRI-Final.pdf
IHME. (2021, December 4). Retrieved from Global Burden of Disease India Compare| Viz Hub: https://vizhub.healthdata.org/gbd-compare/india
IIPS. (2021). National Family Health Survey. International Institute of Population Sciences.
Lancet. (2017). Nations within a nation: variations in epidemiological transition across the states of India, 1990–2016 in the Global Burden of Disease Study. Elsevier Ltd, 2437-2460.
Leonard, S. A., Main, E. K., & Carmichael, S. L. (2019). The contribution of maternal characteristics and caesarean delivery to an increasing trend of severe maternal morbidity. BMC Pregnancy and Childbirth, 1-9.
Temmerman, M., & Mohiddin, A. (2021). Cesarean section: More than a maternal health issue. PLOS MEDICINE, 1-3.
Sandhya Venkateswaran
Alok Kumar Singh



Find on this page
The Centre for Social and Economic Progress (CSEP) is an independent, public policy think tank with a mandate to conduct research and analysis on critical issues facing India and the world and help shape policies that advance sustainable growth and development.