
Do property rights explain health outcomes of adolescent girls in India?
Reading Time: 59 minutesEditor's Note
Support for this research was generously provided by the Omidyar Network. CSEP recognises that the value it provides is in its absolute commitment to quality, independence, and impact. Activities supported by its donors reflect this commitment and the analysis and recommendations found in this report are solely determined by the scholar(s).
This paper was first published on November 27, 2020. Parts of this paper were updated to reflect correct citations and the paper was republished on March 8, 2021.
Abstract
DOWNLOADS
Evidence from existing literature indicates that children, including adolescents, from disadvantaged sections of the society demonstrate adverse health outcomes, ceteris paribus. This, in turn, prevents them from achieving their full economic potential as adults, essentially creating an inter-generational vicious cycle between poor health outcomes and poor access to resources. Using a novel, nationally representative dataset (the Teen Age Girls [TAG] survey) that collected information from adolescent girls (aged 13-19 years) in India, this first-of-its-kind study attempts to explore the link between property rights and health outcomes. We capture information on property rights through one proxy indicator – housing type; health outcomes are captured using age-standardised height and BMI measures. In India, where the right to property and housing are not recognised as fundamental rights, the poor incrementally gain security of tenure, moving from a continuum of insecure housing to full titles. Research from India and other parts of the world shows that a movement towards greater tenure security has been associated with home improvements, and thus type of housing is a strong indicator of security of tenure and therefore property rights, as viewed within a continuum of rights gained incrementally. Our study finds that adolescent girls from households with lower quality houses and fewer household goods fare poorly on health outcome indicators. This creates a space and need for designing and implementing sustainable policy measures that would eventually uplift the overall quality of life of India’s 80 million adolescent girls.
The Property Rights Research Consortium (PRRC), supported by Omidyar Network India, brings together top research institutions undertaking research on various aspects of property rights, land governance and housing issues in India. It aims to develop a multidimensional understanding of property rights through assessing and testing the broad agreement that property rights are vital to development. The larger purpose is to enable evidence- based solutions for securing land, housing and property rights for all Indians. As part of the PRRC, the Centre for Social and Economic Progress examines health as one of the four themes it analyses,[1] focusing on property rights as a pathway to social mobility. The initiative has contributed to the research on property rights, by examining the multidimensional impacts of property rights in India on mobility, health, real estate markets, gender, etc.[2]
Our work focuses on property rights and health in India. There is substantial research on health disparities amongst poor households, and those belonging to the disadvantaged, vulnerable and marginalised sections of the society, in terms of socio-economic profile. The first part reviews literature on the state of property rights in India and presents an analysis of issues pertaining to security of tenure in India. It also examines literature that links tenure security and property rights with type of housing and home improvements both in India and globally. Drawing from this research, this paper examines available data on type of housing as a strong indicator of security of tenure and property rights. We also study literature on the relations between indicators of socio- economic status and health outcomes, among children in particular. The third part uses data from Project Nanhi Kali, a nationally representative dataset that collected information from adolescent girls (13-19 years) in 2016-17 in India, to examine the link between property rights and health outcomes. The fourth and concluding part of this research examines the findings and proposes new areas of research that can inform us better about how property rights influence health outcomes of adolescent girls.
I. Property rights in India
Though the Indian constitution affirmed the right to property as a fundamental right, it was later removed in 1978 through an amendment.[3] India does not recognise the right to housing, despite having ratified the International Covenant on Economic, Social and Cultural Rights in 1979 (Housing and Land Rights Network (HLRN), 2016, p. 1).[4] The Indian state, therefore, possesses enormous power to acquire land, even of those who possess full legal titles. The poor who cannot afford land/ housing and occupy public or private land that they do not possess titles to, are therefore more vulnerable to lose their homes through forced evictions. Government urban policies and programmes that focus on ‘slum free cities’, further increase this risk, as poor habitations are not only viewed as eyesores, but are also considered threats to public health and morality. Evictions that are normalised as essential to development have deep impacts on the urban poor who are vulnerable to eviction and live life with a high sense of insecurity and impermanence (Bhan, 2009; Bhan, Goswami, and Revi, 2013; Ghertner, 2008; Ramanathan, 1996, 2005, 2006).
There is no official data on forced evictions in India. The Housing and Land Rights Network (HLRN), a Delhi based NGO has been collecting some data on forced evictions since 2017 through the National Eviction and Displacement Observatory (NEDO), a network of partner organisations in India. This data is not exhaustive and is based on the limited number of organisations within the NEDO and their access to information. Based on this data, the HLRN reported 213 evictions in 2017, with 53,700 homes destroyed and affecting 2,60,000 people (Chaudhry et al., 2018).[5] In 2018, it reported 218 evictions, with 41,700 homes destroyed and rendering 2,02,000 people homeless (Chaudhry et al., 2019).[6] During both these years, the majority of those evicted were for beautification and development projects — 77 percent in 2017 and 73 percent in 2018; beautification alone accounted for the largest share of evictions — 47 percent of homes destroyed in 2017 and 47 percent of affected persons in 2018 were due to this reason. In its 2018 report, HLRN’s data also revealed that 11.3 million Indians are vulnerable to eviction and potential displacement. Again, this is not an exhaustive figure and is limited by access to data.
Uncertainty about land and property rights forces the poor to postpone their plans in perpetuity (Thara, forthcoming). They refrain from planning for their future and do not make investments to improve their quality of housing and productivity of land, in the fear that an eviction would wipe out their investments. Lack of security propels people to spend time protecting their land/housing (Feyertag et al., 2020) and also in political activities to gain the support of local politicians, thus taking away time from productive work (Thara, forthcoming), or from other essential activities such as childcare (Feyertag et al., 2020). People are also physically vulnerable to violence and injury, as can be seen in India in the many ‘slum fires’ that are often suspected to have been initiated to evict the poor (Chaudhary et al., 2019, pp. 30-31),[7] especially if the groups concerned have little political support (Feyertag et al., 2020; Thara, forthcoming).
The Indian state does provide some housing for the poor and economically weaker sections, but this is largely inadequate and does not address to the massive demand for affordable housing. The Report of the Technical Group on Urban Housing Shortage (TG-12) (2012-2017) estimated the urban housing shortage in India at 18.78 million houses, with 99 percent of the demand from economically weaker sections (EWS) and lower-income groups (LIG).[8] The Working Group on Rural Housing for the 12th Five-year plan estimated rural housing shortage at 43.13 million units.[9] While there is state-wise data on the housing provided under various programs, there is no national-level data on the total housing provided in India each year to the EWS and LIG sections.[10] A good part of the housing provided by the state is often used to displace the poor, offering ‘rehabilitation housing’ in exchange for vacating land within cities for development or beautification projects (Thara, forthcoming). This housing is provided not as a right but as a welfare measure, under the Directive Principles of State Policy (Part IV of the Constitution) which provides for a set of non-enforceable state responsibilities.[11]
II. Tenure security in India
While the poor often live on land they do not own, and do not possess full titles to property, they enjoy varying levels of tenure security.
Tenure security has been defined via multiple modes over the years. Payne (1996, p. 3) defines land tenure as ‘the mode by which land is held or owned, or the set of relationships among people concerning the use of land and its products’, within these frameworks, land tenure relies on the social recognition of use rights vis-à-vis property rights which are state or legally-recognised interests in land or property. (Payne and Durrand-Lasserve, 2012) Fischer (1995) also viewed land tenure as ‘a social relation involving a complex set of rules that governs land use and land ownership’, noting that there is heterogeneity in the access to the ‘bundle of rights’.
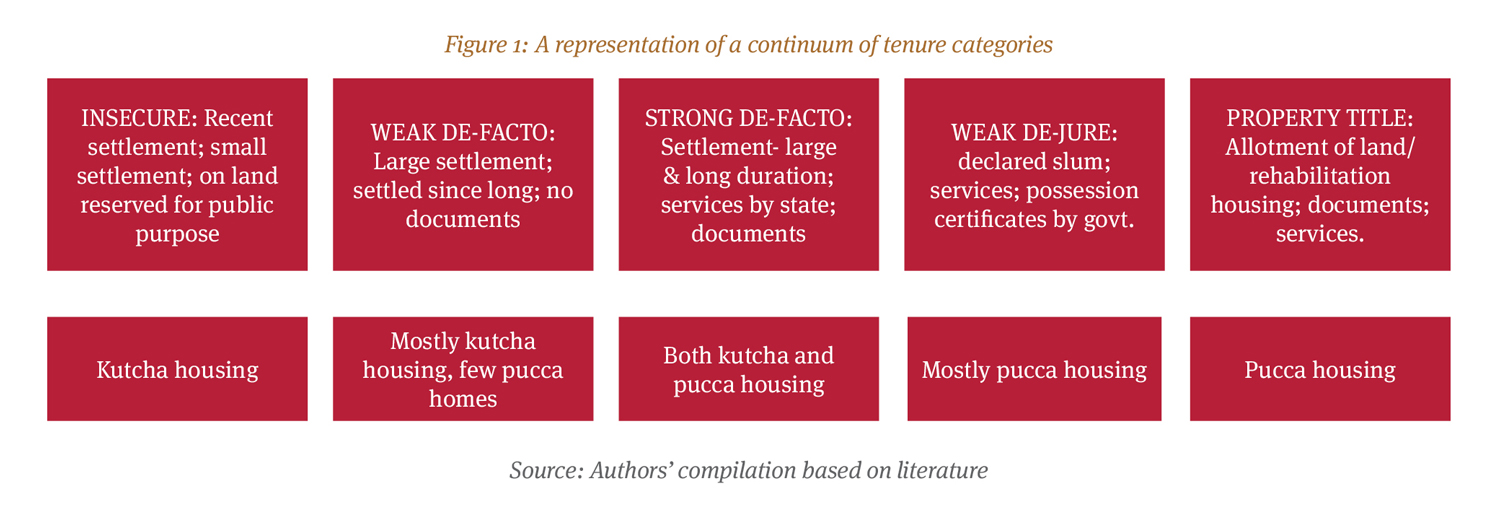
Tenure security is not solely determined by law, and therefore, notions of legal or illegal, formal or informal status, do not apply. It is ‘a relative concept and a matter of perception as well as law’ (Payne, Durrand- Lasserve, & Rakodi, 2009). The poor transition through different stages of tenure security from insecure tenure (with no rights whatsoever and a very high risk of forced eviction) to de-facto rights – i.e., rights in fact (with a perception of security) and finally, progress to achieve de-jure rights – i.e., legal rights of various types, including right to reside, possession certificates, allotment of homes and property titles. Slums and settlements are classified into notified or non-notified slums. Those living in non-notified slums live with insecure tenure, while notified slums enjoy a quasi-legal status, as they are recognised by the state and are also often supplied with public services. Those living in non-notified slums may begin with insecure tenure, but can transition to obtaining de-facto rights through long residence; bigger size of settlement which allows them to gain political support through vote banking; through access to welfare benefits (access to BPL/APL cards); access to public services and infrastructure from the state and/or access to voter identity cards or payment of property tax. Apart from the duration of residence and size of the settlement, the strength of de-facto tenure security also depends on how many people possess such documents in a given slum (Mahadevia, 2010). Access to services such as water, electricity, sanitation and toilets is perceived as an indication of the state’s acceptance of the continued existence of settlements, thus providing de-facto tenure (Paul Strassmann, 1984; Strassmann, 1980).
As Nakamura points out, the strength of political support or lack of it can also determine whether or not a settlement enjoys a weak or strong de-facto tenure (Nakamura, 2014). De-facto tenure is obtained through many factors rather than a single act of the state, and thus results in improved quality of life and social protection. Those having de-facto tenure have a greater perception of secure tenure in comparison with those who possess insecure tenure. Slums that are new, small in size, and/or located on land reserved for public purposes, may not be able to obtain de-facto rights. Those living in de-facto tenure security may enjoy either weak or strong de-facto tenure, depending on the type of land they inhabit and the form of de-facto tenure security they have obtained. (Paul Strassmann, 1984; Strassmann, 1980).
De-facto rights are not only socially recognised, but also recognised by the state. Possession or occupation of land is often considered by the state as providing certain rights to the occupier, based on the duration of possession. In governing land within cities, the Indian state has tended to recognise these rights, often incorporating occupation as a consideration in land planning. Urban sociologists call this “occupancy urbanism” (Benjamin, 2008). Slums and settlements with de-facto rights are recognised by the state as possessing certain rights, especially if they have existed for long periods of time, as this is also legally recognised under the law of adverse possession. The first schedule to the Indian Limitation Act, 1963, provides for a period of 12 years for property owners to approach a court of law to reclaim property taken over through illegal possession against the will of the owner. When the land in question belongs to the state, the prescribed period is 30 years.[12] This law is subject to interpretation by courts, which demand proof of possession and weigh evidence to establish whether the possession was ‘adverse’ to the owner, i.e., with the knowledge and without the consent of the owner. However, the fact that possession is recognised as creating legal rights perforates into everyday law and governance. This can be observed not only in the manner in which the state deals with slums and settlements, but also in its policies on legalising illegal occupation of land that aim to ‘regularise’ illegal constructions and occupations of land (Benjamin & Raman, 2011). This facile conversion of illegal to legal (albeit subject to certain rules and regulations) facilitated by the exchange of money for a change in papers, forces us to think of property law and rights in a far more fluid sense in the Indian context, and not in a rigid sense of either having or not having rights to property. Furthermore, the success of poor groups in asserting claims to land/property is dependent on political configurations at different levels (local, state and national). Therefore, de-facto rights that provide different levels of tenure security are just as important in the Indian context as de-jure or legal rights to property.
De-jure rights are gained when the state confers legal recognition of such housing through slum declaration, certificates of rights/possession certificates, the provision of rehabilitation housing, etc. Just as there are varying grades of de-facto security (weak and strong), de-jure status can be further broken down into quasi-legal status of various types, beginning with slum notification, allotment of slum rehabilitation housing/sites and finally transfer of full property titles. Legalisation of land titles involves amending land laws pertaining to ownership, use and transfer (Mahadevia, 2010). Payne et al. observe that people who benefit from titling programs often seem to have enjoyed ‘a certain level of de-facto tenure security’ in the past (Payne et al., 2009). He suggests that “a starting point maybe to regard every step along the continuum from complete illegality to formal tenure and property rights as a move in the right direction, to be made on an incremental basis.” He also notes that the sharp distinction between formal and informal may be misleading. The notion that all formal or legal land property holders conform to all laws, rules and regulations, is erroneous as the degree of conformity may vary (Payne, 1996).
This progression from one level of tenure to another, normally takes place due to the struggles of the poor who incrementally obtain rights that are manifested through their access to basic services such as water, sanitation and electricity (Das, 2011). Therefore, tenure security is intricately interwoven with access to services, with progressively higher tenure security meaning better access to services. Sociologists have been advocating for policies to provide tenure security to poor households, in this incremental manner, claiming that it would help the poor retain their housing, while an outright provision of property rights may result in them losing their homes to those who can afford to buy them out (Payne et al., 2009). “Secure tenure is the right of individuals and groups to effective protection by the State against forced evictions”, while insecure tenure contains the risk of forced eviction (Durrand-Lasserve & Selod, 2007).[13] Mahadevia (2010) argues that it is important to distinguish between use rights and property. She argues that “the latter is, therefore, a market paradigm of land holding, whereas the former is a welfare approach wherein the right to shelter is extended”. Secure tenure guaranteed by legal rights can therefore accomplish welfare objectives (ibid.).
Varley (1987) points out that while providing legal tenure can benefit urban poor settlements, legalisation alone is not sufficient to enable improvement in the lives of the poor. Providing titles without providing access to infrastructure and services, and other upgrading measures, would not serve the purpose that tenure security is meant to achieve.
III. Tenure security and quality of housing
Providing security of tenure results intangible consequences in the lives of the poor. With stronger tenure, the poor enjoy better access to basic services, a better standard of life and improved economic status (Mahadevia, 2010). Secure tenure alone (Gelder, 2009; Payne 2001) and tenure with income (Payne, 1996) can motivate the poor to invest in improving their homes, which, in turn, can have a range of other positive outcomes, making titling unnecessary. Perceptions of tenure security are important as they influence behaviour and the decisions people make, which have social, economic, and environmental consequences. The Prindex, a research group, has come out with a global assessment of perceived tenure surety for 140 countries. This comparative report collects perceptions data across diverse land governance systems, with differing levels of security tied to legal titles and different sources of property rights, including traditional systems. As per the report, 21 percent of Indians feel insecure about their main property, while 66 percent feel secure. The report further reveals that 22 percent feel insecure about all their properties, while 64 percent feel secure.
In India, the poor live in homes that can be broadly categorised into three types: kutcha housing, pucca housing and semi-pucca housing. Kutcha housing is makeshift housing constructed with materials that last temporarily, for example, mud walls, thatched roofs, or plastic-covered roofs, etc. Pucca housing is built with materials that last, brick and mortar housing with concrete roof. Semi-pucca housing are structures that are built with both permanent and temporary materials. For example, brick and mortar structures with thatched, asbestos, or plastic sheet roofs or with unfinished floors.[14] According to the National Family Health Survey 4 conducted in 2015-16, 0.9 percent of the urban population and 8.1 percent of the rural population live in kutcha housing. Around 13 percent of the urban population and 46.9 percent of the rural population live in semi-pucca housing. Almost 85 percent of the urban population and only 41.2 percent of the rural population lives in pucca housing. The following section of the paper examines evidence both from India and as well as from other parts of the world, which establishes that tenure security (de-facto and de-jure including property titles) motivates poor households to improve their homes.
In Ahmedabad, the Slum Networking Programme (SNP) covered 60 slums and 13,000 households and provided physical infrastructure such as water, electricity and toilets, roads, street lighting and solid waste management; a ‘no demolition guarantee’ of ten years and community-based programmes (including community health centres). Physical infrastructure was provided on an 80-20 basis, with households required to bear 20 percent of the cost. To understand the effects of varying levels of tenure security, a study of six slums under the SNP was conducted in Vasna ward in the south-west part of Ahmedabad, Gujarat, with a sample of 553 households of a total 3,514 households. The six slums were segregated on the basis of tenure into three categories: ‘strong de-facto tenure, weak de-facto tenure and insecure tenure’. This research revealed that settlements with higher tenure security have higher numbers of pucca homes. While 54 percent of households in the insecure tenure category lived in kutcha, or temporary houses, it fell to 39 percent in settlements with weak de-facto tenure and 32 percent in settlements with strong de-facto tenure. While 42 percent of households with strong de-facto tenure lived in pucca housing, it fell to 39 percent in weak de-facto tenure, and only 24 percent in insecure tenure situations (Mahadevia, 2010b). These findings are significant to our study as they reveal that pucca homes have a higher probability of more secure tenure, while kutcha homes have a greater probability of less secure tenure. This is despite the fact that all these settlements had benefitted under the SNP program (Mahadevia, 2010b).
While the six slums with varying tenure security status studied by Mahadevia benefitted from this program, differences in access to both infrastructure and services offered under the SNP persisted on the lines of tenure security. The most pronounced differences were noted in terms of access to water. In slums with strong de-facto tenure, 90 percent of households had individual water supply and only four percent depended on common public taps; in settlements with weak de-facto tenure, 29 percent of households had access to individual water connections and 18 percent depended on public water taps; and with insecure tenure, only 19 percent had individual water taps and 52 percent depended on common public taps. In strong de-facto tenure settlements, all households had access to toilets and 94 percent had access to an individual toilet in their household; in weak de-facto tenure settlements, 86 percent had access to individual toilets, one percent depended on community toilets and five percent did not have access to toilets; and in insecure tenure situations, 69 percent had access to individual toilets, 18 percent used community toilets and 2 percent had no access to toilet (Mahadevia, 2010b). As this data reveals, a greater number of poor households with insecure tenure and weak de-facto tenure did not opt to invest 20 percent in physical infrastructure, despite the government’s 10-year no eviction guarantee. Tenure security, which includes access to basic services, is thus crucial to motivate poor households to invest in their homes and improve from kutcha to pucca structures.
Quality of housing improves when settlements obtain de- jure status even if this is a quasi-legal status. Nakamura, for instance, in his research in Pune, shows that slum residents improve their homes, especially once their stay has exceeded 10 years. This study shows that slum declaration increases the chances of households’ using better materials in constructing their homes by 47 percent and adding a second floor by 78 percent (Nakamura, 2014). It is therefore clear that type of housing is a strong indicator of property rights in the broader sense of the term, including security of tenure as discussed here.
Studies from other parts of the globe also confirm the link between secure tenure and home improvements. In a study of 296 households in squatter settlements in Cartagena, Colombia, Strassman examined home improvements across different population groups. He found that both tenure and access to water encourage owner-occupants to expand and improve their homes (Strassmann, 1980). Thus tenure security or property titles cannot be considered in isolation from access to basic services. In another study conducted in Lima, Peru, Strassman studied 506 households in two impoverished urban neighbourhoods – Popular Urbanisation and Pueblos Jovenes – to compare home improvements by owner- occupants. He suggests that home improvements were motivated more by access to services than any other factor (Strassmann, 1984).
These studies show that providing property rights alone without access to services, cannot motivate home improvements, confirming our definition of property rights as including access to services and basic infrastructure.
Field, in her study of a nation-wide titling program in Peru, found a 68 percent increase in home renovation within four years of titling. (Field, 2005).
Jimenez (1983), in a study of a squatter legalisation program in Tondo, Manila (between 1975 and 1981), also confirmed a similar effect of property rights on home improvement. This legalisation program affected 27,500 households (180,000 individuals) living in 16,500 homes located on 137 hectares of urban government-owned land in Manila’s port area. The project included the provision of individual water connections, road access, sewerage systems, and support for community and health facilities. It rationalised the land tenure system in the area allowing residents the right to buy a lot in the area at a highly subsidised price. Homes were re-blocked minimising dislocation while rearranging homes to conform to regularised lot lines so each home would have access to a communal roadway or footpath and to the main water and sewer lines. Within three months of re-blocking, overall housing quality in Tondo increased by 30 percent to 44 percent. The monetary value of the absolute difference in housing quality before and after re-blocking ranged from about 4,200 pesos to over 6,200 pesos in 1978 (approximately, U.S. $600 to $886 at the time of the study). In comparison to other estimates of changes in the average values of housing in both developing and developed countries, Jimenez concluded that a significant portion of the changes measured in Tondo must be project-induced. Even in the absence of a formal and effective mortgage market, the habitants were able to generate enough resources to make substantial investments in their homes, with the author concluding that the riskiness of investments in homes was lowered by the provision of tenure.
Porio & Crisol (2004) found that residents with tenure security or a promise of titles invested more in improving their homes. Regularised (with de jure rights) homes invested substantially both in home and land while the un-regularised (with de facto rights) improved their homes. Improvement in homes included using more durable building materials such as cement, iron and wood to strengthen homes; while land improvement included fencing of plots with iron grills and planting ornamental plants and fruit-bearing trees.
Examining the impacts of land titling programs such as the World Bank’s Land Administration Program on tenure security and housing consolidation, Reerink and Gelder surveyed 340 households in seven kampongs in Bandung, Indonesia.[15] Housing consolidation was measured on the basis of a composite score representing quality of the floor, the walls, and roof. The sample consisted of 100 titled households; 95 semi-formal tenure households (with traditional ownership rights under adat) and 145 households with informal tenure (squatters on public/ private land). Data was collected from 50 low-income households across seven kampongs. The study found that those ‘with formal tenure live in significantly more consolidated dwellings than informal dwellers’, but found no difference between formal and semi-formal dwellers. Though titling contributed to housing consolidation’, its impact was found marginal. (Reerink & van Gelder, 2010).
Durrand-Lasserve and Selod (2007) argue that “improvements in home environment can have indirect beneficial effects on health of household members.” There are a few studies on the impacts of property rights on health. In Mahadevia (2010b), health outcomes were recorded in one of the six slums chosen for the study. Apart from an improvement in living conditions, improvements in health, education, income, employment status and asset ownership, were also observed. (Mahadevia 2010b).[16] Providing tenure along with infrastructure and services clearly resulted in improved health outcomes, as evident from this study.
Galiani and Schargrodsky (2004) in their study in Buenos Aires, Argentina, have examined the impacts of legal property titles on child health and education. Their study shows, that children living in titled property had better Weight- for-Height scores, lower teenage pregnancy rates, and lower school repetition grades than children living on land without titles. Field (2003), in a study of a Peruvian urban titling programme, finds that providing legal titles resulted in a 22 percent decrease in fertility. She attributes this to improved “bargaining power of women in fertility decisions” due to titling, in addition to “a decrease in the ‘value’ of children since they are no longer needed to secure informal ownership rights or claims to community resources”, and are less “needed for their parents’ old age subsistence”. In the next section, we discuss the link between socio-economic factors and health outcomes.
IV. Socio-economic status and health outcomes
Literature in social sciences has demonstrated a continued interest in SES, especially in demography- related studies. However, there has not been any conclusive evidence on what it definitively represents (Bradley and Corwyn, 2002). It is considered to include a comprehensive list of demographic and economic variables, including but not limited to, caste, religion, occupation, education, income, family size and household composition, parental involvement and education, ownership of a set of assets, and access to facilities or services; some studies also extend the scope of the definition to include parameters like neighborhood and school influences. Further, globally, SES is found to have strong links to developmental outcomes such as health, education and cognitive outcomes. In this research, we refer to SES as a combined measure to represent demographic, economic and social status for a household. The variables considered are discussed in the following sections of this paper.
A number of studies have documented how asset ownership affects health outcomes among children. Simandan (2018) points out that the “subjective experience of social class mediates widely differentiated outcomes for the mental and physical health of upper- class individuals”. Those belonging to the lower classes have fewer resources and thus experience uncertainty and worse outcomes, whereas, the upper-class has greater financial, social and intellectual resources at their disposal, allowing them to have control over their lives (Simandan, 2018). Asset ownership of households determines the household’s SES and, in some sense, can be understood as a measure of wealth. A review of studies were undertaken to determine the relationship between household asset ownership and developmental outcomes of children—undernutrition, access to healthcare services, educational outcomes, schooling and child labour— concluded that asset-building initiatives are a catalyst to enhancing household well-being in developing countries (Chowa et al., 2010).
Boyle et al. (2009) suggest that people’s lack of ability to move upward in the social class system amplifies health inequalities for a household over time and for all subsequent generations. They claim that “healthy are more likely to experience upward social mobility, and those who are less healthy tend to move down the social hierarchy, widening the health gap between higher and lower social classes” (Boyle et al. 2009 pp??). Therefore, children born in disadvantaged households inherit this inequality. Consequently, large inequities in health and health services persist across states, rural and urban areas, and within communities in India (Baru et al., 2010). A community randomised control trial from Zimbabwe has also shown the positive influence of household asset ownership on the well-being of orphaned and vulnerable children (Crea et al., 2012).
In Tanzania, Kafle and Joliffe (2015) use three waves of the National Panel Survey to establish a causal relationship between asset ownership on child health and educational performance. They find that the effect on educational outcomes is asset-specific. Ownership of agricultural assets was found to have an adverse effect on educational outcomes of children.
Another study from Tanzania (Mwageni et al., 2014) looked at SES and health inequalities in rural Tanzania using the Rufiji Demographic Surveillance System (DSS) to find significant gradients in access to assets and health inequalities—infant mortality, under-five mortality, mosquito net ownership—across all wealth quintiles. In studying socioeconomic inequities in health in Tanzania, Schellenberg et al. (2003) found that care-seeking behaviour for children, indicated by child’s illness episode, is worse in poorer families—based on source of income, household assets and the household head’s educational status—than among rich families. Wu et al. (2018) concluded that young adults with more assets and positive net worth have a higher probability of achieving better health outcomes.
Social class health inequalities data of the Office for National Statistics’ Longitudinal Study for England and Wales suggested that social mobility constraints health inequalities (Boyle et al., 2009). Case and Paxson (2006) demonstrate how income inequality is associated with poor child health indicators at birth and this disparity tends to grow more pronounced as children grow older. They show that children from low-income families are more likely to have serious health problems, and these health issues limit children’s economic potential as young adults. While on the one hand, children from the economically weaker section suffer from serious health problems compared to those better off, on the other hand, poorer children fare worse than wealthier children who have the same health concerns. Poor children have access to less and low-quality medical care since their families are ill-equipped to manage their problems, thus worsening their condition. They concluded that improving the physical conditions of children in poor health would lead to their improved economic circumstances later in their lives.
Using the NFHS (1, 2 and 3), Chalasani (2012) provide evidence of wealth-based inequalities in the Indian context. Wealth was determined based on ownership of 13 household assets, including dwelling characteristics. The results indicated that with India’s overall economic growth between 1990 and late 2000s, mortality inequality decreased only in urban areas, although malnutrition increased in rural as well as urban areas.
To understand how household wealth affects health outcomes among children, Bhandari et al. (2002) also observed that children from the affluent section of the society – residing in south Delhi and having socioeconomic characteristics similar to those living in developed countries – had anthropometric indicators closer to the WHO reference range, or are ‘better off’. In the local context, these residents can be considered an outlier towards the higher end of the spectrum.
In India, the literature on caste and wealth status has helped identify and document the disparities that exist across various sections of the society. Coffey et al. (2019) studied the disparity in height of infants across four population groups — Scheduled Caste (SC), Scheduled Tribe (ST), Other Backward Caste (OBC) and General — in rural India. Using decomposition analysis, their paper suggests that differences in children’s height — a crucial indicator of health and future success — can be attributed to differences in the SES of these four groups of the population. They find that socio-economic differences—based on household floor type, mother’s education, household electricity, type of toilet and ownership of phone, radio, TV, refrigerator, bicycle, motorcycle, car and land—can explain the gap in height (lower) among ST children, but not among SC and OBC children. The findings of their study are a departure from research of other population groups where population segregation or the practice of apartheid have been found to be negatively associated with health. In another study of three waves of India’s NFHS (1, 2 and 3), researchers attempted to determine how caste influences delivery of health services based on under-5 mortality and health consumption expenditure (Baru et al., 2010). It concluded that the socially marginalised in India get the least access to preventive and curative health services; they face financial and cultural barriers to utilisation of health services. Their analysis revealed that NFHS-3 (2005-06) shows glaring regional and socio-economic divides in health outcomes — “the lower castes, the poor and the less developed states (bear) the burden of mortality disproportionately” (Baru et al., 2010).
With substantial literature on correlations between SES and health discussed above, we used NFHS-4 data to provide for: (a) caste-wise information on different types of housing, and (b) asset ownership in households based on type of housing.[17] We found that half of the population resides in pucca housing, more permanent structures. Of the remaining, around 43 percent are housed in semi- pucca housing, whereas 7 percent of the population lives in kutcha housing, which are temporary shelter arrangements. As we see in Table 4 in the Appendix, a fewer proportion of people from SC, ST and OBC backgrounds reside in pucca housing (45 percent, 28 percent and 55 percent) compared to 67 percent from the ‘General’ category.[18] Similarly, a smaller section of the remaining population lives in kutcha housing, whereas more people from SC, ST and OBC background live in temporary housing structures. Table 5 in the Appendix suggests that among households that does not possess any household assets, 34 percent are in kutcha structures (59 percent are semi-pucca).[19] As expected, more than 90 percent households that own more than 15 items (maximum being 24) are in pucca houses.
Some literature on homeownership exists from outside India. For instance, Haurin et al. (2002) used four waves of the United States’ National Longitudinal Survey of Youth augmented with Child Data to study the effect of homeownership status on child’s cognitive outcomes and behaviour. Their research design controlled for social, demographic and economic variables that have been traditionally found to influence child outcomes. The study found that in comparison to renting a home, owning a home—an indicator of higher wealth stature—led to higher (a 13 to 23 percent increase) and improved quality of home environment, greater cognitive ability and fewer behavioural issues among children (Huarin et al., 2002).
Ample evidence exists that has established the effect of early-life health on adult circumstances, including an individual’s earning potential and achievement. Lundborg et al. (2014) established that taller people earn more- a “substantial height premium” exists when all other factors are accounted for (also, Currie and Vogl, 2013; Avgeropoulou, 2014). Height has found to be positively associated with cognitive ability, which holds greater value in the labour market (Case and Paxson, 2008). A study from the United States and the United Kingdom shows that taller children have higher cognitive test scores, which in turn determine the height premium in earning in later life (Case and Paxson, 2008).
In addition to the socio-economic status of the adolescent girls, the social determinants of health (SDH) also explain their health outcomes. These determinants are the conditions in an individual’s environment where they are “born, live, learn, work, play, worship, and age” that affects their overall health outcomes (Office of Disease Prevention and Health Promotion [ODPHP, 2020]). An increasing body of evidence has argued in favour of a strong link between these factors and health outcomes in different geographical settings (de Andrade et al., 2015; Adler et al., 2016; Cowling et al., 2014; Kulkarni, 2013) and for various age groups (Ahnquist et al., 2012; Baheiraei et al., 2015; Wilensky & Satcher, 2009), including those of adolescents (Viner et al., 2012). In addition, developing policies that take into consideration various elements of SDH is known to reduce health inequalities (Adler et al., 2016; Penman-Aguilar et al., 2016).
I. The Teen Age Girls (TAG) Survey [20]
To test our research hypotheses, we used a nationally representative novel data set obtained through a primary survey – the Teen Age Girls (TAG) Survey. This survey was conducted during 2016 and 2017, under Project Nanhi Kali, which is jointly managed by Naandi Foundation and K. C. Mahindra Education Trust. The uniqueness of this nationally representative survey lies in the fact that it focused only on various aspects of India’s teenage girls such as their health, education, and most notably, their dreams and aspirations. The survey collected information from 74,000 adolescent girls, aged 13 through 19 years during the survey period, from across 30 states and seven Indian cities, which had a population of more than four million according to the 2011 Census. These cities were Ahmedabad, Bengaluru, Chennai, Hyderabad, Kolkata, Mumbai, and New Delhi. Sample from each state is allocated to its urban and rural areas in a way that it is proportional to its population in these areas, with a minimum of 500 samples from urban areas across all the states. The Ethics Committee of the Institutional Review Board at the L. V. Prasad Eye Institute, Hyderabad, granted approval to Naandi Foundation to carry out the TAG Survey.
The sampling design and sample size allows for producing national- and state-level estimates by various socio-economic groupings, separately for rural and urban areas, as well as city-level estimates. The survey adopted a multi-stage sampling strategy to identify respondents, separately from rural and urban areas. Selection of respondents involved three and four stages, respectively, in rural and urban areas, including seven cities. In rural areas, the first stage involved selecting villages, which were the primary sampling units (PSUs). The second stage comprised of selecting households from within the PSUs that had at least one girl aged 13-19 years. If there were two or more 13-19-year-old girls from the selected households, then in the third stage one girl was randomly selected from such households to be the survey respondent.
All the villages within a state constituted a sampling frame, except for those villages with less than five households, which were excluded. All included villages were first stratified in various regions such that each stratum comprised of villages from neighbouring districts. Further stratification was conducted within each region by village size, based on number of households. The cut-off number applied for stratifying villages within a region by size varied across state and region. Within each village type stratum (based on size), further stratification was applied using a cut-off number that was obtained based on the proportion of SC/ST population. Finally, an implicit stratification was applied within these villages based on ascending order of female literacy. In case a large village (more than 300 households) is selected, an adequate segmentation is carried out first by dividing the village into two or more smaller segments comprising of 100-200 households. Finally, only two segments were selected, which formed the primary sampling unit. Households with at least a respondent within all selected villages or village segments comprised of a sampling frame. From within this frame, a total of 22 households, including two households to account for any non-response, was selected using systematic random sampling.
As mentioned earlier, respondents from urban areas and towns were selected through a four-stage process. First stage comprised of selecting a required number of urban wards, followed by selecting one Census Enumeration Block (CEB) from each ward in the second stage. In the third stage, a required number of households within selected CEBs that had at least one 13-19-year-old girl was selected. In case a selected household had more than one respondent, one such respondent was selected randomly.
A similar step-wise stratification technique, like in the rural areas, was adopted in the urban areas. All the wards across all cities and towns in a state formed a sampling frame. These wards were first stratified into various regions of contagious districts, with implicit stratification carried out based on female literacy. Probability proportional to size (PPS) technique was used to select a required number of wards from each stratum. Only one CEB from among all the CEBs within the selected ward was randomly selected. Further, from all the potential households, with at least one adolescent girl, in the selected CEB, 22 households were selected using systematic random sampling.
Respondents from seven cities were also selected using a four-stage process. In the first stage, a required number of urban wards were selected from all the wards applying PPS technique and implicit stratification based on female literacy. Second stage comprised of selecting two CEBs from the selected urban wards. The next two stages, as well as selection of households, followed exactly the same pattern as in urban areas.
The TAG data set obtained by the study team comprised of approximately 61,600 observations. However, due to missing data and biologically impossible values (discussed later) of the dependent variables, the final sample size of our analysis is about 56,200 observations. In the following section we describe the variables that we have used in our analysis.
II. Variables
Dependent variables: We studied the impact of housing type and other SES related variables on health outcomes using two dependent variables, height-for-age z-scores (HAZ) and BMI-for-age z-scores (BAZ). These variables were computed using standard conversion techniques developed by the World Health Organization’s (WHOs)
AnthroPlus tool, which allows for “assessing growth of the world’s children and adolescents” (WHO, 2009). We discuss this step subsequently.
The TAG survey collected weight, height and hemoglobin data on-site from respondents using a digital weighing scale (in kilograms), the Prestige Stadiometer (in centimeters) and HemoCue Hb 301 analyser, respectively. For the purposes of this study, we have only used weight and height data. In order to reduce error originating either from the surveyor or the measuring instrument, girls’ height and weight were measured three times and recorded under three variables each. We created two new variables, one each for weight and height, by taking the average of the original three variables. For approximately 200 respondents, where weight and height data for one variable was entered as zero, we computed the average using the remaining two non-zero values for weight and height.
We applied the WHO Stata-based macro available to users (WHO, 2009) on input data comprising of girls’ height, weight and age to obtain standardised scores or z-scores for height-for-age and BMI-for-age for adolescent female population aged 13-19 years. The WHO macro does not produce weight-for-age for children beyond 10 years as this indicator “cannot distinguish between height and body mass in an age period where many children are experiencing the pubertal growth spurt and may appear as having excess weight (by weight-for-age) when, in fact, they are just tall” (WHO, 2009, p. 2). These z-scores provide us the distance and direction of a respondent’s measurement from the population mean in units of the standard deviation. These measures are obtained by comparing individual respondent’s growth indicators against growth data from a reference population, using LMS technique (see de Onis et al., 2007; Cole 1990). The standardised measures are used to explore growth and nutritional status (e.g., stunting, overweight) among infants through adolescents. The use of z-scores is recommended as (a) they allow us to compare with a reference population, (b) being a dimensionless quantity, allow for comparisons across age and sex, and (c) are able to compute extreme values. The WHO macro also flags biologically implausible or extreme z-scores for height-for-age (less than -6 or greater than 6) and BMI-for-age (less than -5 or greater than 5), which we dropped from our analysis to reduce outlier influence on estimated coefficients.
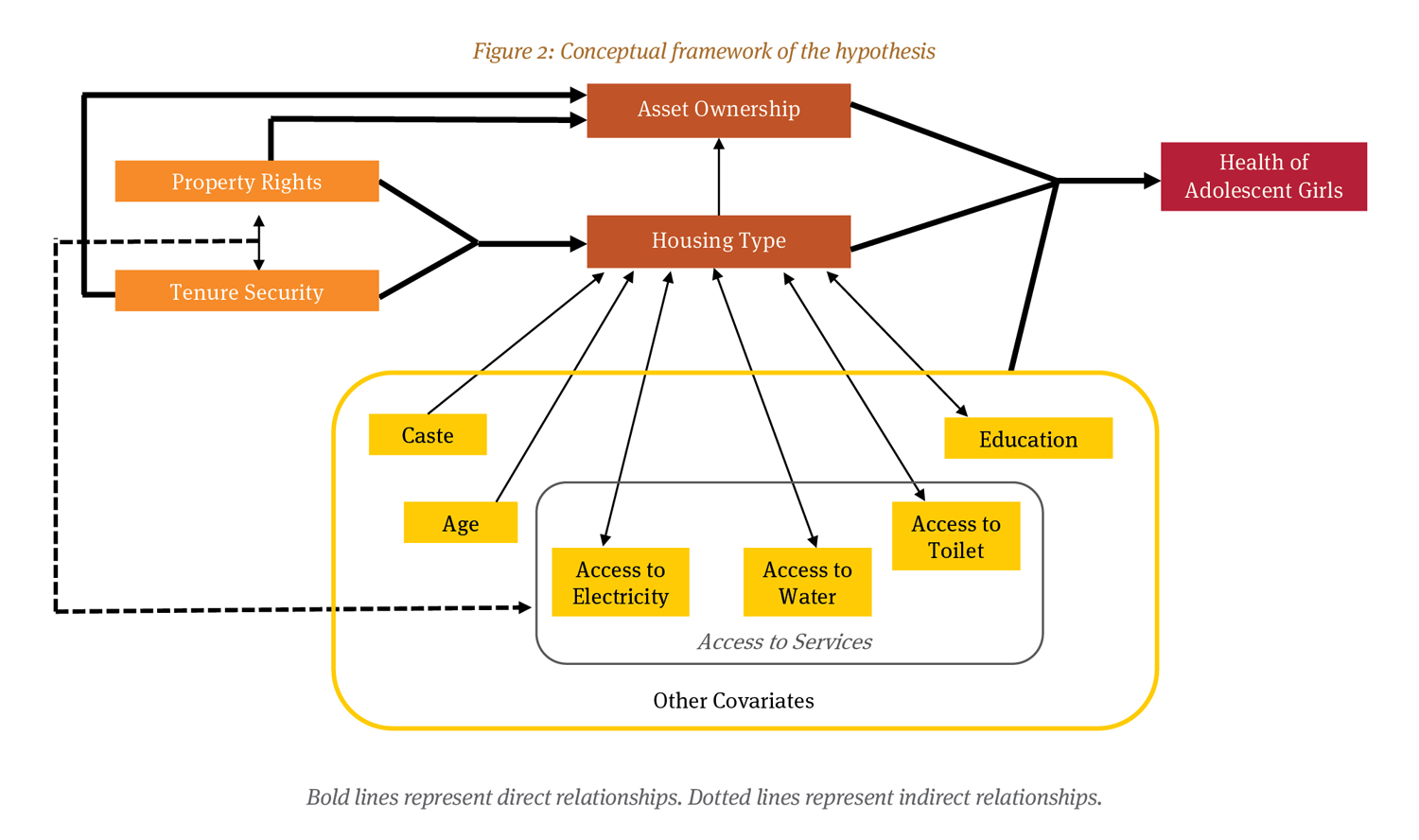
Independent variables: The TAG survey did not ask any direct questions related to property ownership or rights. Therefore, we looked for other ways (variables) to capture the idea of ownership. Based on our review of the extant literature, we believe the type of house is such a candidate variable. In our dataset, house type is a categorical variable comprising of three categories – pucca, semi-pucca and kutcha house. Households with more ownership rights and tenure security are likely to reside in better quality houses (through formal ownership or formal rent agreements etc.). However, the type of house indicates the economic condition of the household as well. Richer families are expected to live in pucca houses, while poorer ones are expected to occupy semi pucca, and kutcha houses. Thus, the effect of house type on health outcomes can be due to the ownership as captured through the quality of the house or the economic condition of the family. If the dimension of economic well-being and wealth is controlled for through some other variable(s), then the residual effect of the type of house on health outcomes can be interpreted to be the effect of the house type and, by proxy, of tenure security and property rights. A well-constructed permanent house not only provides shelter from elements but also provides a sense of security. Therefore, we expect the quality of house and health outcomes to be positively related. The variables through which we attempt to capture the economic condition of the household are a set of variables recording the ownership of around 25 household items and the availability of a toilet within the house premises.
The heterogeneity in material possessions among the households is recorded in a set of binary variables. The survey asked and recorded the ownership of a total of 25 separate items. These items range from smaller value items like chair, fan, watch, to high-cost items like cars. Moreover, there are items like threshers and tractors which are of the nature of capital goods. Considering various aspects of the items (i.e., cost, capital good), we have created five variables to demonstrate item ownership. They include ownership of low-cost items (count), slightly costlier household durables (count), thresher and/or tractor (category), animal cart and car (last two are binary). Sometimes in the literature, a categorical wealth quintile variable is created from this type of item ownership variables. However, we decided against following that path as ownership of a car and ownership of a table fan should not be treated similarly – which is done in the creation of such wealth indices. Another variable that captures economic condition of household is the availability of toilet facilities within the house. This variable captures both the economic condition and health awareness level of the family.
Apart from these, we have included source of lighting in the house, source of drinking water, and other demographic indicators as control variables. Source of lighting can be either electricity, kerosene, solar panels, bio-gas, etc. Given that most (over 95 percent) of the sampled households either used electricity or kerosene to light up their houses, we coded the sources into three categories – electricity, kerosene, and everything else. The survey collected information about the source of drinking water within the household as well. The source of drinking water has two aspects that can affect the health and well-being of the girls. First, if the water is not treated then it could expose the girls to water-borne diseases. Second, if the source of the water is too far away from home, then fetching the water can expose the girls to both physically demanding work and to safety-related issues. However, the survey did not collect any information on the distance of the source or whether the water source is treated or not. Therefore, we decided to capture the heterogeneity in the sources of drinking water through a binary variable – piped water vs everything else. We think that piped water can be considered to be a treated source of drinking water while there are question marks over the other sources (open well, covered well, river, pond, etc.).
Demographic control variables include indicator variables on caste (ST, SC, OBC, and General), religion groups (Hindus, Muslims, Christians, Sikhs, Others), parental education (six ordered categories for both mothers and fathers), number of household members, whether the girl is currently going to school or college and the age of the girl.
Ideally, we would have liked to have a variable that captured the relative position of the girls within the household. The sex of the head of the household, relative number of males and females in the household could have been such variables. But we do not have any such variable in the dataset. Therefore, we decided that the educational qualification of the parents and whether the girls are currently enrolled in a school or college will have to do. There could be many reasons for girls to not be currently enrolled in school or college (not being able to cope with the classes, family does not think education is important for girls). But if the girl is currently enrolled, then that means that not only the girl is able to cope, but the family values their education. This last part, in turn, implies that we can think that such families value the girls as well. In addition, we also believe that a girl’s relationship with the head of the household could determine how a girl is treated within the household. Our analysis included this through a six-category relationship variable.
III. Empirical Strategy
Multiple regression allows us to control for factors which are expected to affect the health outcomes along with the house type and goods ownership variables. Thus, we employ this empirical method for deciphering the association between the health outcomes and the explanatory variables of interest. Our general empirical model is of the following form:
![]()
where the index i stands for each adolescent girl and the index j stands for each PSU. The dependent variable is either the standardised height-for-age or BMI-for-age. Vectors of variables and vectors of coefficients are written in bold in the above equation. Thus, H is a vector of (binary) variables that denote the house type (kutcha, semi-pucca, and pucca, with pucca being the reference or base group); SES is a vector of socio-economic status variables (source of lighting, availability of toilet and piped water in the house, and number of household items owned/possessed by the family); Caste is a vector of (binary) variables that denote caste of the household (SC, ST, OBC, and general, with general being the reference group); and X is a vector of other demographic controls (whether the surveyed girl is currently studying, mother’s and father’s education, relation of the surveyed girl to the head of the household, age of the girl, number of household members, and religion of the head of the household). All models’ parameters are estimated allowing for PSU unobserved heterogeneity through PSU fixed effects.
We estimate several regressions of this form. First, we estimate average differences in adolescent girl’s height (and BMI) by house type by running a regression with the house type as the only indicators. Next, we include controls for caste to see whether the differences in the averages are because people belonging to ST or SC category are more likely to live in poorer quality houses vis-a-vis OBC and General category (the association between caste and house type is shown in the Appendix). Then, as discussed earlier, we include controls for parental education, religion, relationship of the girl to the head of the household, number of household members, current educational enrollment status of and age of the surveyed girl (and its square). Next, a set of indicator and count variables about the household’s SES is included. The indicator variables used to account for household-level SES are ownership of car, and ownership of animal cart. The count variables used are the number of items owned in a set of fourteen relatively low-cost household items,[21] the number of items owned in a set of seven slightly more costly household durables,[22] and ownership of two agricultural equipment (a thresher and a tractor). We use cluster robust standard error estimates where the clustering is done at the PSU level. We use probability weights supplied by the survey dataset in all the estimations. In the next section, we present the findings from our analysis.
I. Descriptive Statistics
Table 1 presents the overall characteristics of our sample. The top portion of this table presents the descriptive statistics for our dependent variables (and the variables from which they are derived), and the bottom portion presents the same for explanatory variables used throughout the study. The average height-for-age z-score is -1.54. This means that, on an average, an adolescent girl in India is almost one and a half standard deviation shorter than their counterparts in the WHO reference group. This shorter average height can be an indicator of the differences in nutrition, genetics, and general living condition. The BMI-for-age difference between Indian adolescent girls and their international counterparts is not as much as that in the height variable. But still, in terms of BMI-for-age, Indian girls underachieve by more than half a standard deviation. Although, height-for-age z-score and BMI-for-age z-score are our main dependent variables, we carried out some additional analysis in terms of height (measured in cms.), weight (measured in kgs.), and BMI of the girls surveyed. The average height of the adolescent girls in India is computed to be just above 151 cms. and the average weight is approximately 44 kgs. The weight of the girls has a relatively large standard deviation of approximately eight kgs. (the coefficient of variation is much larger for weight compared to height – 18 percent and 4.25 percent, respectively). The average BMI is 19.23, which can be considered to be within the normal BMI range of 18.5-24.9, albeit on the lower side. However, a standard deviation of close to three indicates that on the lower side, many girls actually slide into the underweight group.
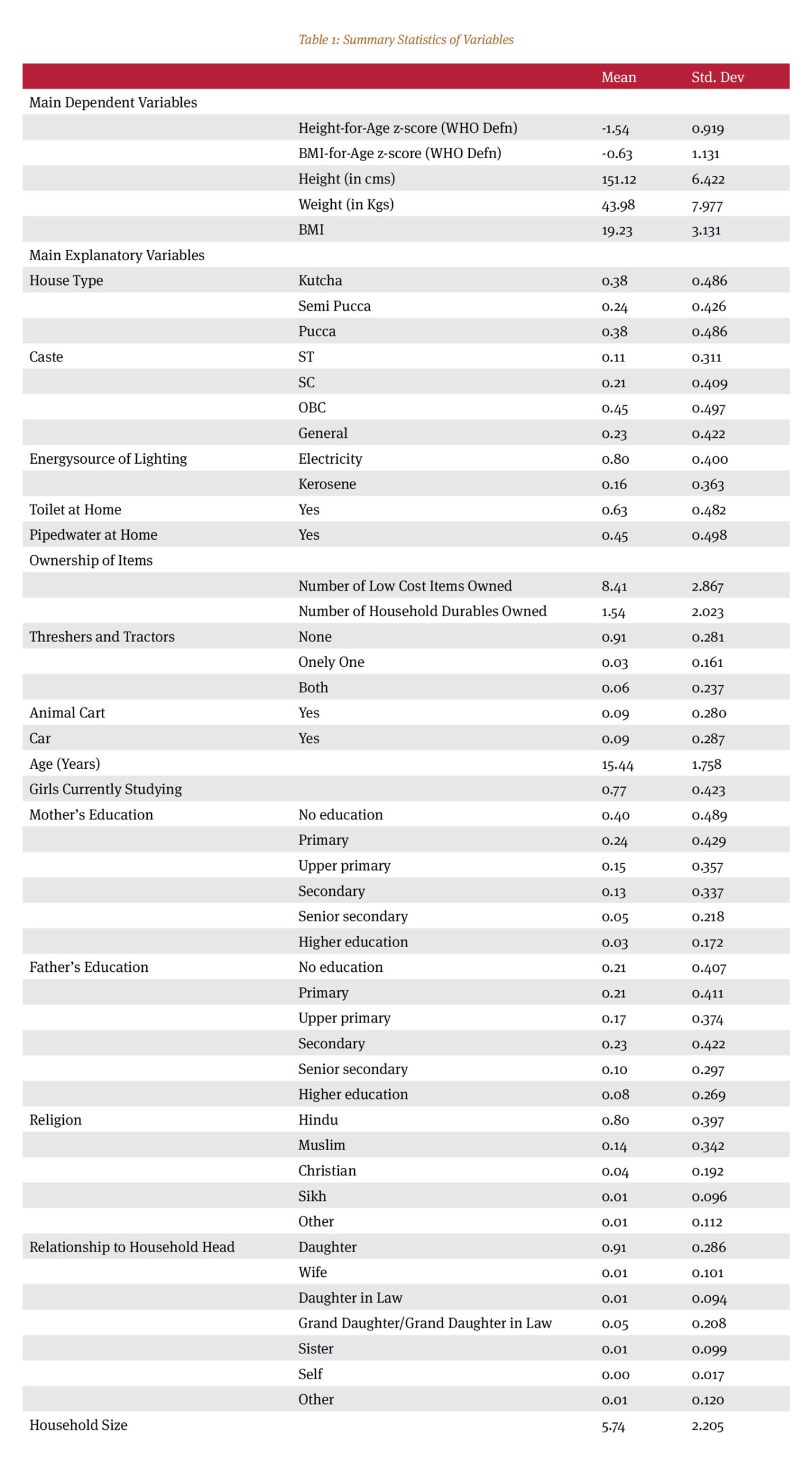
The rest of Table 1 reflects the information available regarding living condition, ownership of household stuff, and demographic characteristics of our sample. Kutcha and pucca house dwellers constitute roughly equal proportion (38 percent each) of the entire sample with the rest living in semi-pucca houses. The caste composition of our sample is 11 percent ST, 21 percent SC, 45 percent OBC, and 23 percent General category. The representation of General caste in our sample is a bit smaller than their share in the national population, according to NSSO data. Recent NSSO surveys estimate this percentage to be close to 30 percent.[23] This gap is filled in by slight over-representation of other three castes, with OBCs accounting for the most of it (around a four-percentage point over-representation). Although caste composition of TAG sample is slightly different from the national averages, religious composition is quite on the mark. Hindus, Muslims, Christians, and Sikhs constitute 80 percent, 14 percent, 4 percent, and 1 percent of the sample, respectively. The rest is constituted by other religions.
Close to 80 percent of the households use electricity as source of energy for household lighting, while 16 percent use kerosene lamps. Around 63 percent of the houses have toilet facilities, whereas 45 percent have piped water facilities at home. On an average, households own around eight relatively low-cost household items, and around one and half of the slightly more costlier household durables and appliances.[24] Animal carts are owned by around 9 percent of the houses and an equal percentage owns cars. Tractors and threshers are owned by households involved in agriculture. Around 3 percent of the sample own only one of these two items, while double of that owns both items. Approximately two-thirds of the sampled girls (77 percent) were currently studying. Around 40 percent of the girls have mothers without any education and the same percentage for the fathers stand at 21 percent. Finally, most (91 percent) of the surveyed girls were daughters of the head of the household. Next, we discuss the results of our estimations.
II. OLS Regression Results
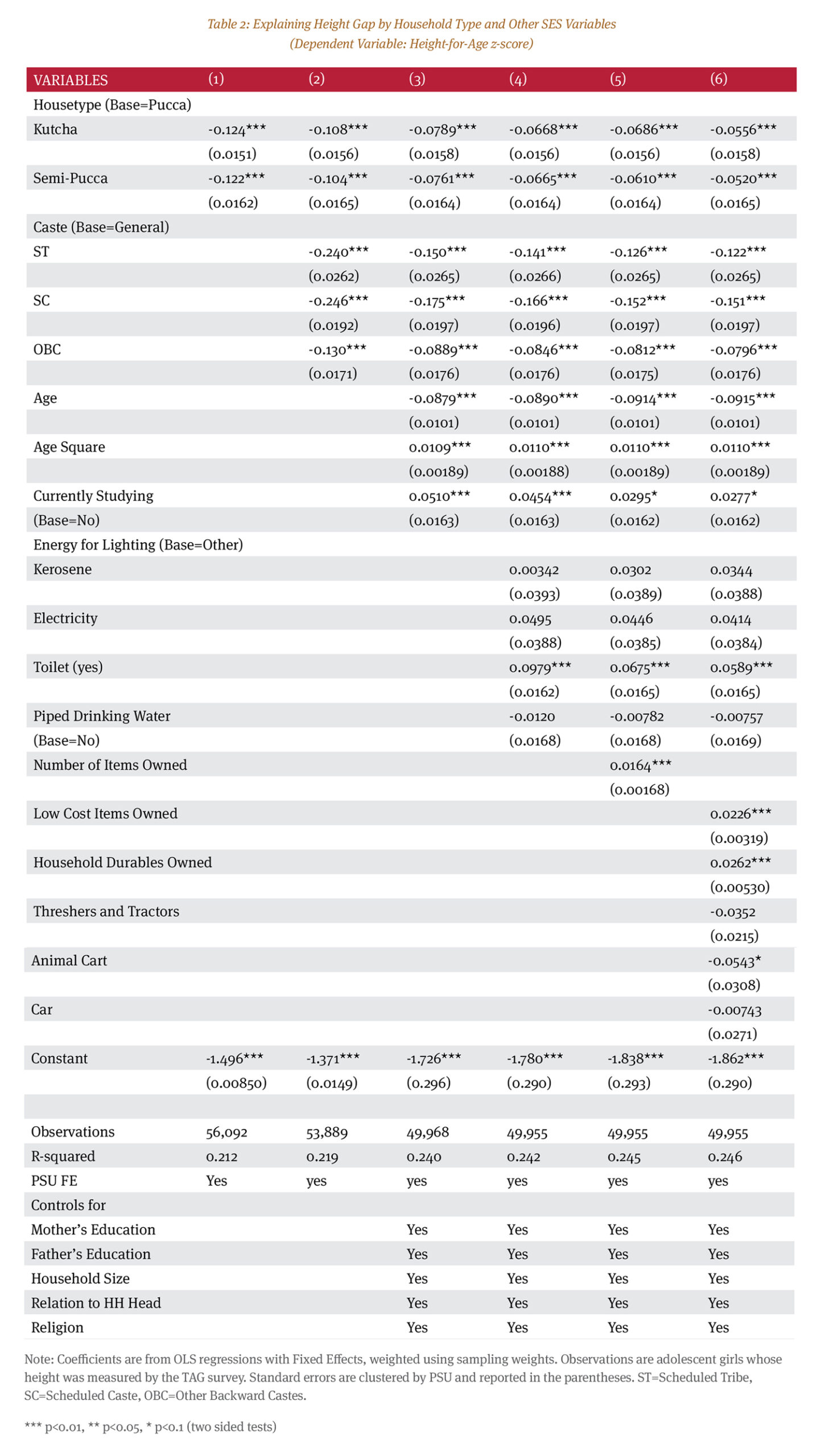
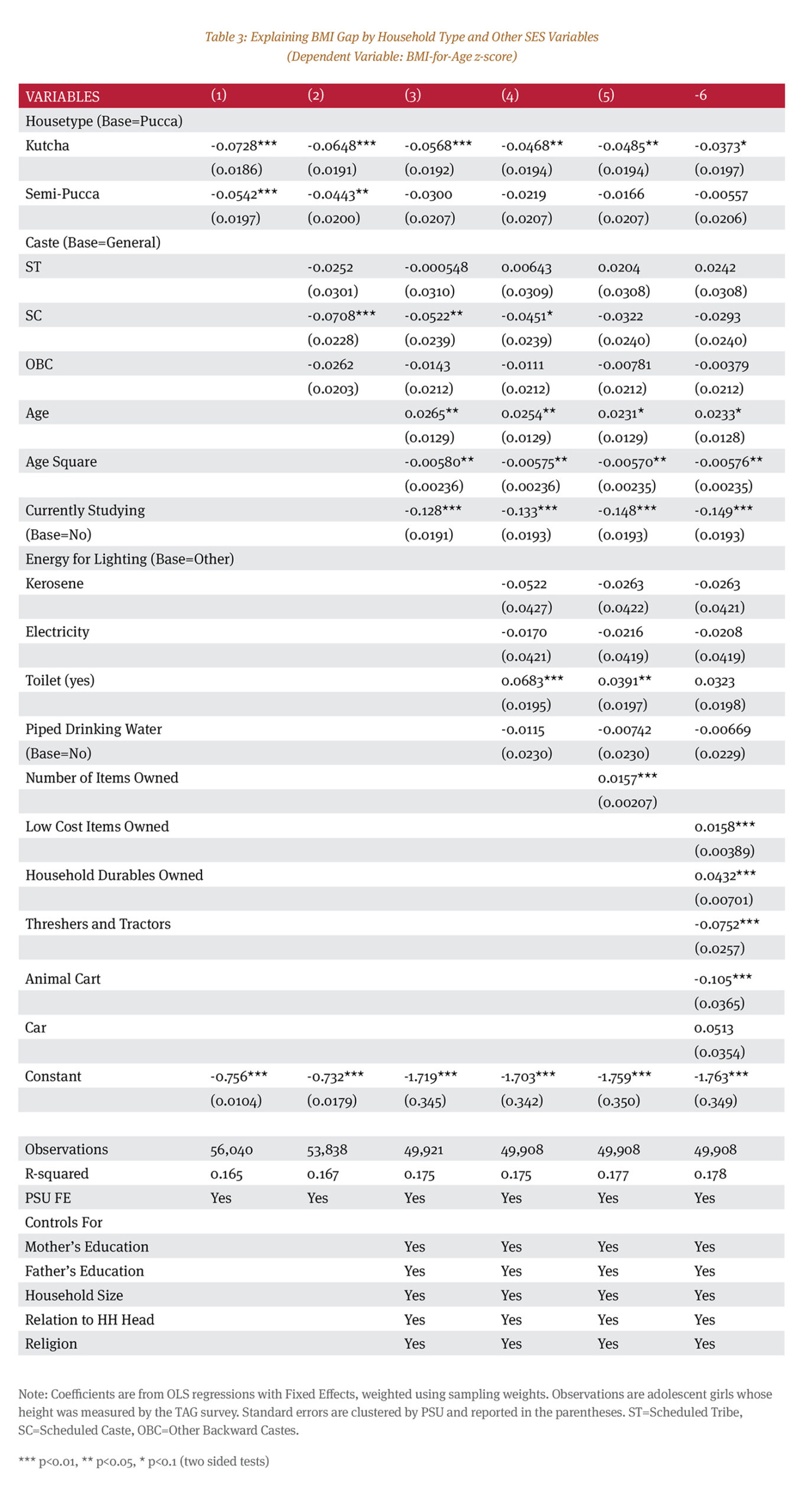
In Tables 2 and 3 we present our main regression results. In column 1 of both tables, we only estimate the expected difference in height-for-age z-score and BMI-for-age z-score for the surveyed girls based on their housing conditions. Those who live in pucca houses are the reference (or base) group. Thus, the intercepts are the estimated height-for-age z-score (Table 2) and estimated BMI-for-age z-score (Table 3) of those girls who live in pucca houses. The estimated coefficients of kutcha and pucca (both are statistically significant in both the tables) show by how much adolescent girls living in these two types of houses underachieve in terms of these two health outcomes relative to the pucca house dwellers. For example, the baseline point estimates (Table 2) tell us that compared to an adolescent girl living in a pucca house, a girl living in a kutcha house is expected to have 0.124 standard deviation lower height-for-age z-score and a girl living in a semi-pucca house is expected to have 0.122 standard deviation lower height-for-age z-score. Similarly, on an average, compared to the reference group, a girl living in a kutcha house and semi-pucca house has 0.073 and 0.054 standard deviation lower BMI-for-age z-score, respectively. As we include other factors which are expected to affect height-for-age z-score, these point estimates keep becoming smaller – signifying that part of the differences are being explained by those other factors.
In column 2 of both the tables, we introduce the caste variables to account for this underachievement through caste discrimination. Health and material underachievement due to caste is a well-documented fact of Indian society. The General category is the reference group here. As expected, the coefficient on all the three lower castes – ST, SC, and OBC – are negative. But while all the three coefficients are statistically significant in Table 2, that is not the case in Table 3. Thus, on an average, girls from these castes underachieve in terms of height-for-age z-score relative to the General category girls. This result persists in all our models. However, although the girls belonging to the SC category statistically significantly underachieve relative to the General category in terms of BMI-for-age z-score, the ST and OBC girls’ underachievement is not statistically significant.
In columns 3, 4, 5, and 6, we progressively include demographic controls and different types of ownership variables. Source of lighting (kerosene lamp, electricity, or other types) and access to piped drinking water at home does not seem to affect either height-for-age or BMI-for- age z-scores – both in the models where we do not include any indicator of wealth (through item ownership) and models where we do. Girls who reported that they are currently studying have a positive and negative effect, respectively, on their height-for-age and BMI-for-age z-scores. However, availability of toilet affects health outcomes positively. When we include detailed controls for item ownership, this positive effect vanishes for BMI- for-age z-scores. Thus, to some extent, the availability of toilet is a proxy for wealth and economic condition of the household, which, when captured through other direct variables, loses its explanatory power at least for BMI-for- age z-scores. For both the dependent variables, ownership of household items has a positive effect on health outcomes. Ownership of these items indicates economic well-being and hence affects the health outcomes positively. The difference between columns 5 and 6 are in how we treat different types of household items vis-à-vis each other.
In column 5, we have a naïve count of all the items – treating all items similarly. The item variable in column 5 thus does not make a distinction between a car and a chair, allocating equal weight to these items. To make this distinction, we group household items into different types based on a rough estimate of their prices and usage. This gives us five variables capturing economic well-being rather than just one. Ownership of threshers and tractors does not seem to affect height-for-age z-scores (although the coefficient is negative, it is not statistically significant), but negatively affects BMI-for-age z-scores. There is a greater probability that these items are owned by relatively well-to-do agricultural households. One way to explain this result is to appeal to the possibility of discrimination against girls within these households. Thus, girls may be deprived of nutrition and care in such households, which results in lower achievement on relevant health outcomes. Ownership of animal cart also negatively affects health outcomes. This may be through poverty pathway (in addition to whatever inter-household discrimination is present). Some households that own animal carts probably earn a living through plying those carts. With widespread mechanisation in all aspects of transportation and agriculture, such livelihood may not be very profitable resulting in an economic disadvantage for the families. And girls from poorer families suffer setbacks in health outcomes. One of the interesting results is the non-existence of any effect of car ownership on health outcomes. This is interesting because car ownership is expected to indicate economic well-being and hence should affect health outcomes positively. One possibility for not finding any significant effect of this variable could be that the ownership of other items captures this dimension already and hence there is no additional effect of car ownership on our variables of interest. Although we have not presented the results here, we have estimated the coefficients of similar models using height measured in centimeters (cms.), weight measured in kilograms (kgs.), sample z-score of height, weight, and BMI as well (Tables 2A and 3A in the Appendix). All the results discussed above (from Tables 2 and 3) hold for these variables as well.
As a robustness check, we also estimated the baseline (column 1 in regression Tables 2 and 3) and the full model (column 6 in Tables 2 and 3) for the rural, urban (excluding the seven major cities included in the survey) and the seven major city sub-samples separately (Tables 2B and 3B in the Appendix). For the dependent variable height-for-age z-score, the results for the rural and urban subsamples are almost similar to what we have presented here, although the coefficients of the house type variables remain no longer statistically significant in the urban sub-sample. In the city sub-sample, only a few variables seem to explain any part of the variation in the dependent variable. The coefficient of constant from city sub-sample is the lowest among the three sub-samples. This coefficient, which is the estimated average height-for-age z-score for a girl with zero values on all the explanatory variables, is a whopping 2.5 standard deviation lower. This sub-sample needs further exploration.
For the dependent variable BMI-for-age z-score, result from the urban sub-sample is similar to what we have found here. In the rural sub-sample, coefficients on the house type variables are not only statistically significant, the sign on semi-pucca is positive. However, the ownership of household items seems to have similar effect as the results presented here. The results from the city sub-sample are contrary to our expectations. Neither the house type nor the caste variable seems to explain the variation in the BMI-for-age z-score in this sub-sample. The two variables that are found to be important (with positive and statistically significant coefficients) for both height-for-age z-score and BMI-for-age z-score are whether the mother had higher education and the ownership of household durables. The effect of mother’s educational achievement on the welfare of the family and the children is a well-documented fact. The ownership of household durables implies better economic condition and hence has a positive effect on the health outcomes. These results are consistent across all our models.
Our main results tell us a generally consistent story. Girls from households that live in poorer quality houses (kutcha or semi-pucca) tend to have adverse achievement on the health outcomes even after controlling for economic condition of the family and caste differences. Thus, even after accounting for those differences, the quality of houses still seems to be a strong predictor of health outcomes for the adolescent girls in India.
We believe that this is a first-of-its-kind study from India that has attempted to address a major evidence gap in terms of linking property rights with health outcomes of adolescent girls, a group that roughly comprises seven percent of the total population (Office of the Registrar General & Census Commissioner, India [ORGI], 2020). Though the TAG survey does not provide us information on the property rights enjoyed by these households, literature that we have discussed earlier establishes a relationship between type of housing and property rights, and between property rights and home improvements. This, therefore, allows us to safely assume that those living in pucca houses in this study have a greater probability of enjoying secure tenure in the least and property rights in the best-case scenario. Similarly, we can safely assume that kuccha houses have a greater probability of having insecure tenure. Our findings on type of housing as influencing health outcomes are significant in that they underline the importance of decent housing to health outcomes. Our research can therefore be interpreted as making a case in the least for the underlying importance of decent housing with adequate access to basic services such as water and toilets. Secure tenure can motivate poor households to improve their homes, and thereby result in positive health outcomes.
In the absence of straightforward data on property rights from India, we have attempted to use a proxy measure – type of house – that strongly indicates property rights, including tenure security (Mahadevia, 2010), to study its impact on adolescent girls’ physical growth measures. As discussed earlier, such growth measures are known to not only have life-long impacts but can also be intergenerational (Mulugeta et al., 2009; Murrin et al., 2012). Adolescence is generally considered as the last window period to take necessary steps to control any intergenerational impact of poor health outcomes (Gebregyorgis et al., 2016; Melaku et al., 2015). We believe this study has produced critical evidence, significantly linking house type with health outcomes, thereby justifying the need for implementing sustainable policy measures today, in order to have a more equitable future.
A significant proportion of existing research from India that has attempted to predict adolescent girls’ growth measures has focused on nutritional and household SES factors (some of which are included in this study). Most of such studies are either based on small sample (Macwana et al., 2017; Rohilla et al., 2014; Goel et al., 2013) or in a specific type of residence such as in rural areas (Coffey et al., 2019). Such study designs limit the generalisability of findings. Our study is a departure from the existing empirical findings; it uses a nationally representative data set, the TAG survey, to test the research hypotheses. Upon comparing simple bivariate cross-tabulations (e.g., caste and house type) from TAG and NFHS-4 data sets, we find some similarity. This provides additional validation regarding the quality of TAG survey data.
Based on the most robust model, which includes full set of controls as well as village-level fixed effects (column 6 in Tables 2 and 3), our analysis indicates that overall, an adolescent girl residing in a kutcha and semi-pucca house compared to a pucca house experience lower height-for-age, almost by 0.05 SD (p < 0.01). Similarly, girls residing in a kutcha house have significantly lower BMI-for-age; 0.04 SD lower BAZ compared to reference group (p < 0.10). Adolescent girls from rural areas demonstrate significantly lower HAZ scores for house type. Those residing in a kutcha and semi-pucca house in rural areas have 0.07 SD lower HAZ score compared to the reference group (p < 0.01). BMI-for-age score is lower for a kutcha house resident from rural area, albeit insignificantly. To our knowledge, we found only one study from India (Pal et al., 2017) that linked stunting (HAZ < -2SD) and thinness (BAZ < -2SD) with house type in a multivariate setup using a rural sample of 839 adolescents aged 10-17 years. Our findings for the adjusted model, based on rural sub-sample of TAG data on HAZ (used to define stunting) significantly diverges, whereas on BAZ (used to define thinness), it is insignificant when compared with Pal et al. (2017).
Lower attainment in growth measures among girls residing in poor quality housing are known to have life- long and intergenerational impact (Aurino et al., 2019; Murrin et al., 2012). For example, height is an established predictor of academic achievement (Magnusson et al., 2006; Spears, 2012), which in turn determines economic well-being (Agerström, 2014; Lundborg et al., 2014), leading to better quality health (Lê-Scherban et al., 2014), all of which are known to have intergenerational impact. Stulp et al. (2015), based on observations collected through three natural settings, “conclude that human height is positively related to interpersonal dominance” (p. 1) and that it may also explain the social status that a ‘tall’ individual enjoys in a society. Height is also a good predictor of self-esteem in an individual, which significantly explains earnings (Drago, 2008). Thus, there are multiple ways through which an individual’s height could explain overall well-being and satisfaction in life (Salahodjaev & Ibragimova, 2020; Coste et al., 2012).
While we have not included nutrition, personal eating preference, physical activity and a host of other explanatory variables in our analysis, they nonetheless significantly determine growth measures from across various settings. Wassie et al. (2015), based on a community-centered cross-sectional study of adolescent girls from Ethiopia, concluded that increasing the variety in dietary intake and participating in a community-based nutrition programme decrease the odds of poor HAZ and BAZ scores. Unhealthy food consumption pattern and sedentary lifestyle are strong predictors of overweight and obesity, a finding that is common across various countries (Costa et al., 2019; Dixit et al., 2014; Goel et al., 2013; Rohilla et al., 2014; Adesina et al., 2012)
Ownership of household items generally speaks volumes about the economic well-being of a family, thereby affecting health outcomes positively. Findings from our study significantly confirm gains in HAZ and BAZ scores among the owners of low-cost items and household durables. This finding resonates with similar findings on predicting nutritional status among children and adolescents from Bangladesh (Rousham & Khandakar, 2016), Gambia (Juwara et al., 2016), Gaza Strip (Abudayya et al., 2011), and Macedonia (Stojanoska et al., 2014). On the other hand, respondents from the household that owned an animal cart compared to those that did not, report lower height-for-age (-0.05 SD, p < 0.10) and BMI- for-age z-scores (-0.11SD, p < 0.01). Threshers and tractor ownership also significantly predicted lower BAZ score (p < 0.01). Lower growth measures among adolescent girls across these groups, be it rich or poor (reflected by ownership of threshers and tractors, or animal cart), point to another dimension in our society. It is likely that girls, in general from any households are treated differentially, compared to boys. This has been highlighted in studies from Tanzania (Kafle & Joliffe, 2015) and the Unite States (Roberts & Warren, 2017). Differential treatment could include poor dietary provision, which, when sustained for a long time period is known to reduce growth measures.
Access to a toilet facility within household positively impacts adolescent girl’s height-for-age z-scores, with higher upward movement among urban respondents. Pal et al. (2017) study from India and Mulugeta et al. (2009) study from Ethiopia demonstrates the importance of access to a toilet facility. Both these studies illustrate that lack of a toilet facility is significantly associated with thinness and stunting. Evidently, girls who do not have household access to toilets are travelling outside of their homes to defecate in the open, which is known to negatively impact anthropometric indicators (Chakrabarti et al., 2020; Chattopadhyay et al., 2019; Ahmadi et al., 2018). While controlling open defecation remains a priority for the central government, even though the campaign formally ceased on October 2, 2019, evidence indicates that we are far from reality (Yadavar, 2019). Gupta et al. (2019), based on a 2018 survey of four North Indian states, concluded that even though the construction of toilets had increased under the Swachh Bharat Mission, open defecation still continues to be a concern. This problem can only be successfully addressed if there is a nationwide Information, Education and Communication (IEC)-based campaign that promotes use of latrine (Coffey et al., 2014).
Caste continues to explain adolescent girl’s height. Girls from the lower castes – SC, ST, and OBC – suffer from reduced height-for-age z-scores, demanding corrective measures. Girls from Scheduled Caste suffer disproportionately, as has also been established by Venkaiah et al. (2002). Previous studies have explored several pathways through which height of lower caste girls can further explain change in learning outcomes (Aurino et al., 2019) to dietary intake pattern (Seshadri et al., 2016). Most existing evidence indicates that caste is a significant predictor of adolescents’ nutritional status (Degarege et al., 2015; Madjdian et al., 2018; Singh & Bansal, 2017).
As discussed earlier, parental education, either one of the parents or combined, plays a critical role in determining their child’s physical growth measures. Compared to no education, HAZ scores progressively increased with both mother’s and father’s level of education from primary to higher education, Mother’s level of education registered greater gain on HAZ scores. Similarly, mother’s education level also significantly improved BMI-for-age z-scores from secondary level onwards. Educated parents are in a better position to decide on various factors that impact physical growth, from dietary pattern and its nutritional content, to involvement in physical activities.
Limitations
Limitations to our study mostly emanated from the use of the TAG survey dataset. Thus far, only one round of the TAG survey has been conducted during 2016 and 2017. The cross-sectional nature of the dataset does not allow us to observe trends over time. Perhaps, with further rounds conducted we will be able to conduct a robust analysis of how evolution in housing type and property rights impact adolescent girls’ health outcomes. The sample represents female adolescents aged 13-19 years. We, therefore, cannot extend our findings for the male cohort in the same age- group in India.
In addition, no variables in the dataset capture direct or distinct information that would allow us to determine the status of a household’s property rights or security of tenure. Thus, we have resorted to establishing the relationship between tenure security (as a proxy for property rights) and housing type using globally available literature. Further, information on whether the dwelling is owned or rented by the household is not available; this would have been a more refined indicator of property rights. Other existing datasets, such as the Prindex data, which has better information on property rights and ownership, does not include any health indicators.
The TAG survey captures height, weight and haemoglobin levels as the only indicators of health. Thus, height-for- age and BMI-for-age are the most suitable variables for analysis in this context. Weight-for-age is not applicable for this particular age group. Furthermore, data on genetic factors, such as parental BMI and health conditions, which could impact girls’ health is not available.
Data on additional aspects of household demographics such as, gender composition of siblings, social status of girls within a household and primary occupation or type of employment in a household are not available. Including these variables in the regression model would have made our analysis even more robust. In the future, additional waves of TAG survey could include some of these missing variables, including retrospectively, provided conducting survey among the first wave of sample households (as in the India Human Development Survey, various rounds).
Conclusion
The central findings of our analysis are that health outcomes (age-adjusted standardised height and BMI) of adolescent girls in India are systematically lower for those living in poorer quality houses and systematically higher for those in families with ownership of more household goods. Based on the existing literature, we interpret that the type of house is a satisfactory indicator of property rights and tenure security. Thus, we conjecture that girls from households with tenure security fair better in terms of the standard health outcomes relative to girls from households without such security. Adolescent health outcomes strongly predict an individual’s future health conditions. A healthy labour force is not only more productive but also aids in spending a lot less on healthcare. Resources thus generated could be invested in the general well-being of the society. In addition, adolescent girls of today are also the prospective mothers of tomorrow. A healthy mother has a much higher likelihood of bearing a healthy child. Thus, these outcomes are not only contemporaneously important, but have strong intergenerational implications as well. Unfortunately, within the policy arena, the adolescent age group is one of the neglected subsets of the population. Therefore, on the one hand, we need to do more research on the pathways through which property rights and tenure security affects the adolescent girl’s health outcomes and, on the other hand, we need to pay more attention to these linkages within the policy discourse.
The issue of property rights and tenure security of poor households has been approached in the policy space, using a rights-based approach of the right to housing and shelter, or as enabling the accrual of capital through housing that can be used to raise loans and improve the economic opportunities of the poor. Both these approaches miss the health dimensions of decent housing, even if the rights-based approach is broader, and focuses on the human experience of homelessness and the indignity and life-threatening potential of inadequate housing.[26] Our research emphasises the health dimensions of housing, and therefore the potential for affordable housing to provide benefits that are not just economic but also improve human capabilities and, in turn, human achievements.
Our research also points to the provision of tenure security as a solution to the problem of poor housing, within a context of inadequate state resources and the meagre supply of affordable housing. However, this requires a paradigm shift from the current approach of viewing slums and settlements as eyesores and obstacles to development. Poor housing, unsanitary conditions of living and the environmental consequences of slums and settlements such as garbage and open defecation, have been perceived as threats to public health and mortality (Gilbert, 2007). Urban programs that offer affordable housing have been used to remove the poor from within cities and displace them in the peripheries, in ghettoes of sorts, with even poorer access to basic services. Such programs often recreate slums, albeit vertically, in apartment buildings, far away from the city and therefore from sources of lucrative employment. This reveals a myopic view of housing as the mere provision of shelter, which can then be arranged in any part of the city, ignoring both the tremendous upheaval of displacement and the effects of relocation in spaces that provide fewer services and fewer economic prospects (Thara, forthcoming). Mahadevia, for instance, reveals the poor quality of rehabilitation housing provided by the state and the lack of services in such housing (Mahadevia et al., 2013). Kamath reveals how slum dwellers provided with rehabilitation housing have to again negotiate with local political representatives to obtain access to services, which takes place incrementally over years (Kamath, 2012). Thara, in her research in the biggest rehabilitation housing area in Bangalore, reveals how residents, despite their political negotiations, do not have access to piped water and sanitation more than two decades after rehabilitation (Thara, forthcoming). Even during the implementation of the Pradhan Mantri Awas Yojana (launched in 2015), which emphasises the provision of housing in situ (on the spot where slums are originally located), evictions for city beautification have persisted unabated as reported by the HLRN in 2017 and 2018 (Chaudhry et al. 2018, 2019). This is bound to have tangible consequences on the evicted poor, much beyond the mere loss of housing, to a deterioration in conditions of life, lack of access to basic services such as water and sanitation, fall in wages/income, increased travel time, etc. all of which are bound to impact their health. As Mahadevia argues, housing is not the mere provision of shelter but also includes access to services such as water, electricity and sanitation (Mahadevia, 2010). Providing housing, without access to services, as has been evidenced in several slum rehabilitation programs, will therefore not enable people to achieve better health outcomes.
Over the years, a formidable mechanism of slum rehabilitations has been established to address the problem of slums and settlements in India. However, available research on tenure security shows that the poor need nothing more than tenure security to invest in home improvements. We are not the first to point this out, urban sociologists have proposed tenure security as a simple and effective solution to affordable housing requiring low investment by the state and fewer resources (Banerjee, 2002; Kundu, 2009; Mahadevia, 2010; Mahadevia, Joshi, and Sharma 2009). This is specifically in the context of evidence that reveals that a majority of forced evictions in India are for city beautification projects (see discussion on the HLRN reports mentioned in part one). The trade- off between beautifying cities and providing urban poor housing should be, therefore, one that is easier to make, as it is not only in the interests of the larger good, but also results in multiplier effects enabling effective poverty reduction, enabling economic empowerment, and most importantly, improving the capabilities of people through positive outcomes on health.
However, addressing the need for planned housing and ownership requires a paradigm shift in the ways in which the urban poor are perceived both by the state and other actors. It also requires confronting the fear of an apocalypse, of overgrowth and proliferation that is out of control (Gilbert, 2009). This calls for a strong political resolve that can ensure inclusive growth and equitable distribution of resources while withstanding the onslaught of the real estate sector, bureaucrats and political representatives who have a stake in freeing expensive land of its poor inhabitants. Most importantly, allowing for greater upward social mobility of the disadvantaged sections of the society merits a commitment to property rights as integral to enabling equal citizenship.
Abudayya, A., Shi, Z., Abed, Y., & Holmboe-Ottesen, G. (2011). Diet, nutritional status and school performance among adolescents in Gaza Strip (Vol. 17, Issue 3).
Adesina, A. F., Peterside, O., Anochie, I., & Akani, N.
A. (2012). Weight status of adolescents in secondary schools in port Harcourt using Body Mass Index (BMI). Italian Journal of Pediatrics, 38(1), 1–7. https://doi. org/10.1186/1824-7288-38-31
Adler, N. E., Glymour, M. M., & Fielding, J. (2016). Addressing social determinants of health and health inequalities. JAMA, 316(16), 1641-1642.
Agerström, J. (2014). Why does height matter in hiring? Journal of Behavioural and Experimental Economics, 52, 35–38. https://doi.org/10.1016/j.socec.2014.06.002
Ahmadi, D., Amarnani, E., Sen, A., Ebadi, N., Cortbaoui, P., & Melgar-Quiñonez, H. (2018). Determinants of child anthropometric indicators in Ethiopia. BMC Public Health, 18(1), 1–9. https://doi.org/10.1186/s12889-018-5541-3
Ahnquist, J., Wamala, S. P., & Lindstrom, M. (2012). Social determinants of health–a question of social or economic capital? Interaction effects of socioeconomic factors on health outcomes. Social science & medicine, 74(6), 930-939.
Aurino, E., Schott, W., Behrman, J. R., & Penny, M. (2019). Nutritional Status from 1 to 15 Years and Adolescent Learning for Boys and Girls in Ethiopia, India, Peru, and Vietnam. 38, 899–931. https://doi.org/10.1007/s11113-019- 09557-8
Avgeropoulou, E. (2014). The Impact of early childhood conditions on future labour outcomes: Does the early-life health and nutritional status affect future earnings into young adulthood? A case study of the Cebu Metropolitan Area, Philippines.
Baheiraei, A., Bakouei, F., Mohammadi, E., Montazeri, A., & Hosseni, M. (2015). The social determinants of health in association with women’s health status of reproductive age: a population-based study. Iranian Journal of Public Health, 44(1), 119.
Banerjee, Banashree. 2002. “Security of Tenure in Indian Cities.” Pp. 37–58 in Holding Their Ground: Secure Tenure for the Urban Poor in Developing Countries, edited by A. Durand-Lasserve and L. Royston. Earthscan Publications Limited: London.
Baru, R., Acharya, A., Acharya, S., Kumar, A. S., & Nagaraj, K. (2010). Inequities in access to health services in India: caste, class and region. Economic and political Weekly, 49-58.
Benjamin, S. (2008). Occupancy Urbanism: Radicalizing Politics and Economy beyond Policy and Programs. International Journal of Urban and Regional Research, 32(3), 719–729. https://doi.org/10.1111/j.1468- 2427.2008.00809.x
Benjamin, S., & Raman, B. (2011). Illegible Claims, Legal Titles, and the Worlding of Bangalore. Revue Tiers Monde, 206(2), 37–54. https://doi.org/10.3917/rtm.206.0037
Bhan, Gautam, Amlanjyoti Goswami, and Aromar Revi. 2013. The Intent to Reside: Spatial Illegality, Inclusive Planning, and Urban Social Security.
Bhan, Gautam. 2009. “‘This Is No Longer the City I Once Knew’. Evictions, the Urban Poor and the Right to the City in Millennial Delhi.” Environment and Urbanization 21(1):127–42.
Bhandari, N., Bahl, R., Taneja, S., Onis, M. D., & Bhan, M. K. (2002). Growth performance of affluent Indian children is similar to that in developed countries. Bulletin of the World Health Organization, 80, 189-195.
Boyle, P. J., Norman, P., & Popham, F. (2009).
Social mobility: evidence that it can widen health inequalities. Social Science & Medicine, 68(10), 1835-1842.
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual review of psychology, 53(1), 371-399.
Case, A., & Paxson, C. (2006). Children’s health and social mobility. The Future of Children, 151-173.
Case, A., & Paxson, C. (2008). Stature and status: Height, ability, and labour market outcomes. Journal of political Economy, 116(3), 499-532.
Chakrabarti, S., Singh, P., & Bruckner, T. (2020). Association of Poor Sanitation with Growth Measurements Among Children in India. JAMA Network Open, 3(4), e202791. https://doi.org/10.1001/ jamanetworkopen.2020.2791
Chalasani, S. (2012). Understanding wealth-based inequalities in child health in India: a decomposition approach. Social science & medicine, 75(12), 2160-2169.
Chattopadhyay, A., Sethi, V., Nagargoje, V. P., Saraswat, A., Surani, N., Agarwal, N., Bhatia, V., Ruikar, M., Bhattacharjee, S., Parhi, R. N., Dar, S., Daniel, A., Sachdev, H. P. S., Singh, C. M., Gope, R., Nath, V., Sareen, N., de Wagt, A., & Unisa, S. (2019). WASH practices and its association with nutritional status of adolescent girls in poverty pockets of eastern India. BMC Women’s Health, 19(1), 89. https://doi.org/10.1186/s12905-019-0787-1
Chaudhry, Shivani, Deepak Kumar, Anagha Jaipal, and Aishwarya Ayushmaan. 2019. Forced Evictions in India in 2018: An Unabating National Crisis. New Delhi.
Chaudhry, Shivani, Swapnil Saxena, Madhulika Masih, Deepak Kumar, and Aishwarya Ayushmaan. 2018. Forced Evictions in India in 2017: An Alarming National Crisis. New Delhi.
Chaudhry, Shivani, Swapnil Saxena, Madhulika Masih, Deepak Kumar, and Aishwarya Ayushmaan. 2018. Forced Evictions in India in 2017: An Alarming National Crisis. New Delhi.
Chowa, G., Ansong, D., & Masa, R. (2010). Assets and child well-being in developing countries: A research review. Children and Youth Services Review, 32(11), 1508-1519.
Coffey, D., Deshpande, A., Hammer, J., & Spears, D. (2019). Local social inequality, economic inequality, and disparities in child height in India. Demography, 56(4), 1427-1452.
Coffey, D., Gupta, A., Hathi, P., Khurana, N., Spears, D., Srivastav, N., & Vyas, S. (2014). Revealed Preference for Open Defecation Evidence from a New Survey in Rural North India. Economic & Political Weekly, 49(38), 43–55.
Cole T. J. (1990). The LMS method for constructing normalized growth standards. European Journal of Clinical Nutrition, 44(1), 45–60.
Costa, C. S., Rauber, F., Leffa, P. S., Sangalli, C. N., Campagnolo, P. D. B., & Vitolo, M. R. (2019). Ultra- processed food consumption and its effects on anthropometric and glucose profile: A longitudinal study during childhood. Nutrition, Metabolism and Cardiovascular Diseases, 29(2), 177–184. https://doi. org/10.1016/j.numecd.2018.11.003
Coste, J., Pouchot, J., & Carel, J.-C. (2012). Height and Health-Related Quality of Life: A Nationwide Population Study. The Journal of Clinical Endocrinology & Metabolism, 97(9), 3231–3239. https://doi.org/10.1210/ jc.2012-1543
Cowling, K., Dandona, R., & Dandona, L. (2014). Social determinants of health in India: progress and inequities across states. International Journal for Equity in Health, 13(1), 1-12.
Crea, T. M., Lombe, M., Robertson, L. A., Dumba, L., Mushati, P., Makoni, J. C., & Gregson, S. (2013). Asset ownership among households caring for orphans and vulnerable children in rural Zimbabwe: The influence of ownership on children’s health and social vulnerabilities. aids Care, 25(1), 126-132.
Curley, J., Ssewamala, F., & Han, C. K. (2010). Assets and educational outcomes: Child Development Accounts (CDAs) for orphaned children in Uganda. Children and Youth Services Review, 32(11), 1585-1590.
Currie, J., & Vogl, T. (2013). Early-life health and adult circumstance in developing countries. Annu. Rev. Econ., 5(1), 1-36.
Das, V. (2011). State, Citizenship and the Urban Poor. Citizenship Studies, 15(3–4), 319–333. https://doi. org/10.1017/CBO9781107415324.004
de Andrade, L. O. M., Pellegrini Filho, A., Solar, O., Rígoli, F., de Salazar, L. M., Serrate, P. C. F., … & Atun, R. (2015). Social determinants of health, universal health coverage,
and sustainable development: case studies from Latin American countries. The Lancet, 385(9975), 1343-1351.
de Onis, M., Onyango, A. W., Borghi, E., Siyam, A., Nishida, C., & Siekmann, J. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization, 85(9), 660–667. https://doi.org/10.2471/blt.07.043497
Degarege, D., Degarege, A., & Animut, A. (2015). Undernutrition and associated risk factors among school age children in Addis Ababa, Ethiopia Global health. BMC Public Health, 15(1), 375. https://doi.org/10.1186/s12889- 015-1714-5
Dixit, S., Singh, J. v., Kant, S., Agarwal, G. G., Dubey, A., & Kumari, N. (2014). A cross-sectional study on predictors and significance of eating behaviour of adolescent girls. Vulnerable Children and Youth Studies, 9(1), 10–16. https://doi.org/10.1080/17450128.2013.804971
Drago, F. (2008). Self-esteem and earnings (No. 3577; IZA Discussion Papers). http://hdl.handle. net/10419/35097www.econstor.eu
Durrand-Lasserve, A., & Selod, H. (2007). The Formalisation of Urban Land Tenure in Developing Countries. In S. V. Lall, M. Freire, B. Yuen, R. Rajack, & J.-J. Helluin (Eds.), Urban Land Markets: Improving Land Management for Successful Urbanization (pp. 101–132). Dordrecht: Springer. https://doi.org/10.1007/978-1-4020- 8862-9
Feyertag, J., Childress, M., Flynn, R., Langdown, I., Locke, A., & Nizalov, D. (2020). Comparative Report. Comparative Report: A Global Assessment of Perceived Tenure Security from 140 Countries. London. https://doi.org/10.1007/978- 3-663-11897-8_2
Field, E. (2003). Fertility Responses to Land Titling: The Roles of Ownership, Security and the Distribution of Household Assets (Issue October).
Field, E. (2005). Property Rights and Investment in Urban Slums. Journal of the European Economic Association, 3(May), 279–290.
Fischer, J. (1995). Local land tenure and natural resources management systems in Guinea. Research findings and policy Options series. Madison: University of Wisconsin, Land Tenure Center.
Galiani, S., & Schargrodsky, E. (2004). Effects of land titling on child health. Economics and Human Biology, 2(3), 353–372. https://doi.org/10.1016/j.ehb.2004.10.003 Gilbert, Alan. 2007. “The Return of the Slum: Does Language Matter?” International Journal of Urban and Regional Research 31(4):697–713.
Gebregyorgis, T., Tadesse, T., & Atenafu, A. (2016). Prevalence of Thinness and Stunting and Associated Factors among Adolescent School Girls in Adwa Town, North Ethiopia. International Journal of Food Science. https://doi.org/10.1155/2016/8323982
Gilbert, Alan. 2009. “Extreme Thinking about Slums and Slum Dwellers: A Critique.” SAIS Review XXIX (1):35–47.
Goel S, Kaur T, & Gupta M. (2013). Increasing Proclivity for Junk Food among Overweight Adolescent Girls in District Kurukshetra, India. In International Research Journal of Biological Sciences (Vol. 2, Issue 3). www.isca.in
Grinstein-Weiss, M., Yeo, Y. H., Irish, K., & Zhan, M. (2009). Parental assets: A pathway to positive child educational outcomes. J. Soc. & Soc. Welfare, 36, 61.
Gupta, A., Khalid, N., Desphande, D., Hathi, P., Kapur, A., Srivastav, N., Vyas, S., Spears, D., & Coffey, D. (2019). Changes in Open Defecation in Rural North India: 2014- 2018 (No. 12065). www.iza.org
Haurin, D. R., Parcel, T. L., & Haurin, R. J. (2002). Does homeownership affect child outcomes? Real Estate Economics, 30(4), 635-666.
Jimenez, E. (1983). The Magnitude and Determinants of Home Improvement in Self-Help Housing: Manila’s Tondo Project. University of Wisconsin Press Journals Division, 59(1), 70–83.
Juwara, A., Huang, N., Chien, L.-Y., & Chen, H.-J. (2016). Stunting and weight statuses of adolescents differ between public and private schools in urban Gambia. International Journal of Public Health, 61, 717–726. https://doi.org/10.1007/s00038-016-0836-6
Kafle, K. R., & Dean, J. (2015). Effects of asset ownership on child health indicators and educational performance in Tanzania (No. 330-2016-13960).
Kamath, L. (2012). New Policy Paradigms and Actual Practices in Slum Housing: The Case of Housing Projects in Bengaluru. Economic & Political Weekly, 47(47/48), 76–86.
Kim, Y., & Sherraden, M. (2011). Do parental assets matter for children’s educational attainment? Evidence from mediation tests. Children and Youth Services Review, 33(6), 969-979.
Kulkarni, M. (2013). Social determinants of health: The role of neighbourhoods, psychological factors and health behaviours in predicting health outcomes for the urban poor in India. Journal of health psychology, 18(1), 96-109.
Kumar, A. (2014). Estimating rural housing shortage. Economic and Political Weekly, 74-79.
Kundu, A. (2012). Report of The Technical Group on Urban Housing Shortage (TG-12) (2012-2017). Ministry of Housing and Urban Poverty Alleviation, Government of India.
Kundu, Amitabh. 2009. “Access to Basic Amenities and Urban Security.” in India: Urban Poverty Report 2009. Oxford.
Lê-Scherban, F., Roux, A. V. D., Li, Y., & Morgenstern, H. (2014). Does academic achievement during childhood and adolescence benefit later health? Ann Epidemiol, 24(5), 344–355. https://doi.org/10.1016/j.annepidem.2014.02.008
Lundborg, P., Nystedt, P., & Rooth, D. O. (2014). Height and earnings: The role of cognitive and noncognitive skills. Journal of Human Resources, 49(1), 141-166.
Macwana, J. I., Mehta, K. G., & Baxi, R. K. (2017). Predictors of overweight and obesity among school going adolescents of Vadodara city in Western India.
International Journal of Adolescent Medicine and Health, 29(3). https://doi.org/10.1515/ijamh-2015-0078
Madjdian, D. ́onya S., Azupogo, F., Osendarp, S. J. M., Bras, H., & Brouwer, I. D. (2018). Socio-cultural and economic determinants and consequences of adolescent undernutrition and micronutrient deficiencies in LLMICs: a systematic narrative review. Ann. N.Y. Acad. Sci, 1416(1), 117–139. https://doi.org/10.1111/nyas.13670
Magnusson, P. K. E., Rasmussen, F., & Gyllensten, U. B. (2006). Advance Access publication. International Epidemiological Association International Journal of Epidemiology, 35, 658–663. https://doi.org/10.1093/ije/dyl011
Mahadevia, D. (2010). Tenure security and urban social protection – findings and policy implications in India (forthcoming), 41(4).
Mahadevia, D., Datey, A., & Mishra, A. (2013). Foisting Mass Housing on the Poor: Lessons from Social Audit of BSUP (No. 21).
Mahadevia, Darshini, Rutul Joshi, and Rutool Sharma. 2009. Approaches to the Lands for the Urban Poor. Working paper no. 2, Centre for Urban Equity, Ministry of Housing and Urban Poverty Alleviation.
Melaku, Y. A., Zello, G. A., Gill, T. K., Adams, R. J., & Shi,Z. (2015). Prevalence and factors associated with stunting and thinness among adolescent students in Northern Ethiopia: A comparison to World Health Organization standards. Archives of Public Health, 73(1), 1–11. https://doi.org/10.1186/s13690-015-0093-9
Mulugeta, A., Hagos, F., Stoecker, B., Kruseman, G., Linderhof, V., Abraha, Z., Yohannes, M., & Samuel, G. G. (2009). Nutritional Status of Adolescent Girls from Rural Communities of Tigray, Northern Ethiopia. Ethiop.J.Health Dev., 23(1), 5–11.
Murrin, C. M., Kelly, G. E., Tremblay, R. E., & Kelleher, C. C. (2012). Body mass index and height over three generations: Evidence from the Lifeways cross- generational cohort study. BMC Public Health, 12(1), 1–11. https://doi.org/10.1186/1471-2458-12-81
Mwageni, E., Masanja, H., Juma, Z., Momburi, D., Mkilindi, Y., Mbuya, C., & de Savigny, D. (2005). Socio-economic status and health inequalities in rural Tanzania: evidence from the Rufiji demographic surveillance system. Measuring health equity in small areas, 39-52.
Nakamura, S. (2014). Land Tenure, Politics and Perception: A Study of Tenure Security and Housing Improvement in Indian Slums. University of Michigan. https://doi.org/10.1080/14768320500230185
Office of Disease Prevention and Health Promotion [ODPHP]. (2020). Social determinants of health. Washigton, D.C.: U.S. Department of Health and Human Services. https://www.healthypeople.gov/2020/topics- objectives/topic/social-determinants-of-health, accessed November 5, 2020.
Office of the Registrar General & Census Commissioner, India (ORGI). (2020). C-13 single year age returns by residence and sex. New Delhi: ORGI.
Pal, A., Pari, A. K., Sinha, A., & Dhara, P. C. (2017). Prevalence of undernutrition and associated factors: A cross-sectional study among rural adolescents in West Bengal, India. International Journal of Pediatrics and Adolescent Medicine, 4(1), 9–18. https://doi.org/10.1016/j. ijpam.2016.08.009
Payne, G. (1996). Urban Land Tenure and Property Rights in Developing Countries: A Review of Literature.
Payne, G. (2001). Urban land tenure policy options: Titles or rights? Habitat International, 25(3), 415–429. https://doi.org/10.1016/S0197-3975(01)00014-5
Payne, G. and Durand-Lasserve, A. (2012). Holding On: Security of Tenure – Types, Policies, Practices, and Challenges. Research paper prepared for the expert group on Security of Tenure convened by the Special Rapporteur, Office of the United Nations High Commissioner for Human Rights. See: https://www.ohchr.org/Documents/Issues/Housing/SecurityTenure/Payne-Durand-Lasserve-BackgroundPaper-JAN2013.pdf?fbclid=IwAR0HAr0Cc-
Payne, G., Durand-Lasserve, A., & Rakodi, C. (2009). The limits of land titling and home ownership. Environment and Urbanization, 21(2), 443–462. https://doi. org/10.1177/0956247809344364
Penman-Aguilar, A., Talih, M., Huang, D., Moonesinghe, R., Bouye, K., & Beckles, G. (2016). Measurement of health disparities, health inequities, and social determinants of health to support the advancement of health equity. Journal of public health management and practice: JPHMP, 22(Suppl 1), S33.
Porio, E., & Crisol, C. (2004). Property rights, security of tenure and the urban poor in Metro Manila. Habitat International, 28(2), 203–219. https://doi.org/10.1016/ S0197-3975(03)00068-7
Ramanathan, Usha. 1996. “Displacement and the Law.” Economic And Political Weekly 31(24):1486–91.
Ramanathan, Usha. 2005. “Demolition Drive.” Economic And Political Weekly 12(July):3607.
Ramanathan, Usha. 2006. “Illegality and the Urban Poor.” Economic And Political Weekly 41(29):3193–97.
Reerink, G., & van Gelder, J. L. (2010). Land titling, perceived tenure security, and housing consolidation in the kampongs of Bandung, Indonesia. Habitat International, 34(1), 78–85. https://doi.org/10.1016/j. habitatint.2009.07.002
Roberts, E., & Warren, J. R. (2017). Family structure and childhood anthropometry in Saint Paul, Minnesota in 1918. Hist Fam, 22(2–3), 258–290. https://doi.org/10.1080/1 081602X.2016.1224729
Rohilla, R., Rajput, M., Rohilla, J., Malik, M., Garg, D., & Verma, M. (2014). Prevalence and correlates of overweight/obesity among adolescents in an Urban City of North India. Journal of Family Medicine and Primary Care, 3(4), 404. https://doi.org/10.4103/2249-4863.148127
Rousham, E. K., & Khandakar, I. U. (2016). Reducing health inequalities among girls and adolescent women living in poverty: The success of Bangladesh. Annals of Human Biology, 43(2), 115–121. https://doi.org/10.3109/030 14460.2016.1141985
Salahodjaev, R., & Ibragimova, N. (2020). Height and Life Satisfaction: Evidence from Russia. Applied Research in Quality of Life, 15, 219–237. https://doi.org/10.1007/s11482-018-9672-6
Schellenberg, J. A., Victora, C. G., Mushi, A., De Savigny, D., Schellenberg, D., Mshinda, H., & Tanzania IMCI MCE Baseline Household Survey Study Group. (2003). Inequities among the very poor: health care for children in rural southern Tanzania. The Lancet, 361(9357), 561- 566.
Seshadri, S. R., Parab, S., Bhor, N., & Latha, N. (2016). What we ate then and what we eat now: a grandmother’s tale (No. 2).
Simandan, D. (2018). Rethinking the health consequences of social class and social mobility. Social Science & Medicine, 200, 258-261.
Singh, N., & Bansal, N. (2017). Assessment of nutritional status of adolescent girls in an urban slum area. International Journal of Home Science, 3(2), 310–312. www.homesciencejournal.com
Spears, D. (2012). Height and cognitive achievement among Indian children. Economics and Human Biology, 10(2), 210–219. https://doi.org/10.1016/j.ehb.2011.08.005
Stojanoska, B. B., Janevska, N. N., Matveeva, N., Zafirova, B., & Cadikovska, E. (2014). Growth parameters and nutritional status in relation to socioeconomic status of Macedonian adolescents. Contributions / Macedonian Academy of Sciences and Arts, Section of Biological and Medical Sciences, 35(1), 189–197.
Strassmann, P. W. (1984). The timing of urban infrastructure and housing improvements by owner occupants. World Development, 12(7), 743–753. https:// doi.org/10.1016/0305-750X(84)90085-8
Strassmann, W. P. (1980). Housing improvement in an opportune setting: Cartagena, Colombia. Land Economics, 56(2), 155–168. https://doi.org/10.2307/3145859
Stulp, G., Buunk, A. P., Verhulst, S., & Pollet, T. v. (2015). Human Height Is Positively Related to Interpersonal Dominance in Dyadic Interactions. PLOS ONE, 10(2), e0117860. https://doi.org/10.1371/journal.pone.0117860
Thara, Kaveri (forthcoming), In Search of Home: Citizenship, Law and the Politics of the Poor, Cambridge University Press.
Varley, A. (1987). The Relationship between Tenure Legalization and Housing Improvements: Evidence from Mexico City. Development and Change, 18(3), 463–481. https://doi.org/10.1111/j.1467-7660.1987.tb00281.x
Venkaiah, K., Damayanti, K., Nayak, M. U., & Vijayaraghavan, K. (2002). Diet and nutritional status of rural adolescents in India. European Journal of Clinical Nutrition, 56, 1119–1125. https://doi.org/10.1038=sj. ejcn.1601457
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., & Currie, C. (2012). Adolescence and the social determinants of health. The Lancet, 379(9826), 1641-1652.
Wahi, N. (2015). The Fundamental Right to Property in the Indian Constitution. SSRN Electronic Journal, (2661212). https://doi.org/10.2139/ssrn.2661212
Wang, Y., Chen, H.-J., & Wang, Y. (2012). Use of percentiles and z-scores in anthropometry. In Victor R. Preedy (Ed.), Handbook of Anthropometry: Physical Measures of Human Form in Health and Disease (1st ed., pp. 29–48). Springer- Verlag. https://doi.org/10.1007/978-1-4419-1788-1_2
Wassie, M. M., Gete, A. A., Yesuf, M. E., Alene, G. D., Belay, A., & Moges, T. (2015). Predictors of nutritional status of Ethiopian adolescent girls: a community based cross sectional study. BMC Nutrition, 1(1), 20. https://doi. org/10.1186/s40795-015-0015-9
WHO. (2009). WHO AnthroPlus for personal computers manual: Software for assessing growth of the world’s children and adolescents. Geneva: WHO. Accessed http:// www.who.int/growthref/tools/en/
Wilensky, G. R., & Satcher, D. (2009). Don’t Forget About The Social Determinants Of Health: Although important for all age groups, factors not related to medical care are particularly salient for the healthy development of children. Health Affairs, 28(Suppl1), w194-w198.
Wu, S., Wang, X., Wu, Q., & Harris, K. M. (2018).Household financial assets inequity and health disparities among young adults: Evidence from the national longitudinal study of adolescent to adult health. Journal of health disparities research and practice, 11(1), 122.
Yadavar, S. (2019). After 4 Years of Swachh Bharat, Open Defecation Down 26 Percentage Points, But Toilet Use Does Not Match Construction Spree. https://www. indiaspend.com/after-4-years-of-swachh-bharat-open- defecation-down-26-percentage-points-but-toilet-use-does-not-match-construction-spree-false-claims-evident/
Zhan, M., & Sherraden, M. (2003). Assets, expectations, and children’s educational achievement in female-headed households. Social Service Review, 77(2), 191-211
FOOTNOTES
[1] The four themes analysed by the initiative are – a. Property Rights as a Pathway to Social Mobility – Health, Education, Gender and Media Sensitivity to Property Rights; Property Rights & Housing in India; Property Rights, Regional Connectivity and India’s Strategic Investments in the Neighbourhood; & Property Rights & Judicial Reforms.
[2] Research papers produced by the initiative include: Mobility and tenure choice in urban India (A. Dutta, S. Gandhi, and Richard K. Green; March 2020); Too slow for the urban march: Litigations and real estate market in Mumbai, India (S. Gandhi, V. Tandel, A. Tabarrok, and S. Ravi; January 2019); Are slums more vulnerable to the COVID-19 pandemic: Evidence from Mumbai (S. Patranabis, S. Gandhi, and V. Tandel; April 2020); COVID-19 is a wakeup call for India cities where radical improvements in sanitation and planning are needed (Gregory F. Randolph, and S. Gandhi; April 2020); Why is India’s real estate market stagnating (V. Tandel, and S. Gandhi; April 2020); Migrants aren’t streaming into cities, and what this means for urban India (Gregory F. Randolph, and S. Gandhi; July 2019); Gender and Property Rights: lesser-known aspects of matriliny in North East India. Forthcoming research includes analysis on Vacant Housing in India; Accelerating Land Acquisition Abroad to Enhance India’s Regional Connectivity; Property Rights and Judicial Reforms; and Media Sensitivity to Property Related Conflicts in India.
[3] The Indian Constitution adopted on 26 January 1950 provided for the right to property as a fundamental right under Article 19 (1) (f), subject to restrictions by the state in public interest under Article 19 (6) and Article 31 provided for compensation in case of acquisition. However, as Courts enforced this property right, invalidating several laws aimed at social and economic reform, including land reform laws, the right to property was removed vide the 44th Constitutional amendment in 1978. (Wahi, 2015).
[4] Land and property rights are recognised as important to the reduction of poverty and the empowerment of women, and therefore included in the Sustainable Development Goals 2015 (SDGs).
[5] The HLRN’s partner organisations for the 2018 report on forced evictions in 2017 included : Information and Resource Centre for the Deprived Urban Communities, Chennai; Ghar Bachao Ghar Banao Andolan, Mumbai; Habitat and Livelihood Welfare Association, Mumbai; Ghar Hakka Sangharsh Samitee, Navi Mumbai; Deen Bandhu Samaj Sahyog, Indore; Slum Jagatthu, Bengaluru; Centre for the Sustainable Use of Natural and Social Resources, Bhubaneswar; Montfort Social Institute, Hyderabad; Adarsh Seva Sansthan, Jamshedpur; National Hawkers’ Federation, Kolkata; Voluntary Health Association of Punjab, Chandigarh; ActionAid Association, Jaipur; National Alliance of Peoples’ Movements; Kalpvriksh; and, Land Conflict Watch.
[6] In its 2019 report on forced evictions in 2018, HLRN’s partner organisations were : Adarsh Seva Sansthan; Affected Citizens of Teesta; Association of Urban and Tribal Development; Beghar Adhikar Abhiyan; Campaign for Housing and Tenurial Rights (CHATRI); Centre for Research and Advocacy; Centre for the Sustainable Use of Natural and Social Resources; Ghar Bachao Ghar Banao Andolan (GBGBA); Habitat and Livelihood Welfare Association; Information and Resource Centre for the Deprived Urban Communities (IRCDUC); Land Conflict Watch; Madhya Pradesh Nav Nirman Manch (MPNNM); Montfort Social Institute; Nagrik Sangharsh Morcha; Narmada Bachao Andolan; NIDAN; Paryavaran Mitra; Paryavaran Suraksha Samiti; Pehchaan; Prakriti; Rahethan Adhikar Manch (Housing Rights and Human Rights Group); Save Mon Region Federation; Shahri Gareeb Sangharsh Morcha; Slum Jagatthu; Video Volunteers; & Vigyan Foundation.
[7] The HLRN has a separate section on loss of housing due to fires and notes that though some fires were caused by accident, such as cylinder blasts and short circuits, in most cases, reasons for the fire could not be ascertained, indicating that fires could have been used to evict the poor.
[8] These estimates are based on the NSS 65th round data and the 2011 census data. This data included households living in kutcha housing; obsolescent homes, congested homes, and those in homeless condition. Of the total 18.78 million, 56 percent of demand was from the Economically Weaker Sections, 40 percent from low-income groups and only 4 percent from medium and high-income groups (Amitabh Kundu 2012).
[9] However, this data has been criticised as problematic as it relied on old data sets of the 11th Five-year plan (Kumar 2014).
[10] Data on housing provided is available on various programs, for instance, under the Jawaharlal Nehru National Urban Renewal Mission’s Basic Services for the Urban Poor (JNNURM, BSUP), the Rajiv Awas Yojana (RAY), the PMAY, etc. In addition to these schemes, state governments also provide for housing under state schemes. We did not find concise data that regroups housing provided under all these programs, schemes and the regular allotment of residential land. This is one exercise that may be undertaken in the future to bring about more transparency in the allotment of housing for the poor.
[11] Article 39 (a) provides that the state will direct policy towards securing for Indian citizens, the right to an adequate means of livelihood and the distribution of ownership and control over material resources of the community to serve common good.
[12] Articles 27, 64 & 65 of the Act provide for private property, while Articles 25 and 112 of the Act. Those claiming adverse possession must prove uninterrupted possession, sole occupancy and an element of hostility, occupying and using the land against the owner’s wishes. A 2017 judgement of the Supreme Court in Dagadabai Vs. Abbas (CA83/2008) further makes it imperative that those claiming adverse possession must first ‘admit ownership of the true owner’ and must include the true owner in the case filed for adverse possession.
[13] General Comment No. 7 on the Right to Adequate Housing (E/C.12/1997/4) adopted by the United Nations Committee on Economic, Social and Cultural Rights in 1997, defines eviction as ‘the permanent or temporary removal against their will of individuals, families and/or communities from the home and/or the land they occupy, without the provision of, and access to, appropriate forms of legal or other protection’ (COHRE, 2003).
[14] As per definition followed by major surveys conducted in India, including the NSS and NFHS
[15] Titled households are recognised by the 1960 Basic Agrarian Law (BAL). Households with semi-formal tenure claim rights under the traditional adat law are not recognised by BAL but still possess a semi-formal status, as they are recognised as ‘legitimate claims for formalisation’. Those under adat law are distinct from squatters on state or private land to which they have no legal claim.
[16] Mahadevia refers to data obtained from MHT and Saath, the NGOs implementing the SNP in Ahmedabad.
[17] International Institute for Population Sciences - IIPS/India and ICF. 2017. National Family Health Survey NFHS-4, 2015-16: India. Mumbai: IIPS.
[18] NFHS-4 classifies caste in the following five categories: SC, ST, OBC, None of the Above and Don’t Know. For the purpose of this analysis, we have considered ‘None of the Above’ as the ‘General’ category.
[19] 24 assets also listed NFHS-4 and TAG data (except Landline phone): Mattress, Pressure cooker, Chair, Cot/bed, Table, Electric fan, Radio/transistor, Black &White T.V, Color T.V, Sewing machine, Mobile telephone, Internet, Computer/laptop, Refrigerator, Air conditioner (AC)/Air cooler, Washing machine, Watch/clock, Bicycle, Motorcycle/scooter, Animal drawn cart, Car, Water pump, Thresher, and Tractor
[20] This section is based on the Teen Age Girls Report, available at: https://www.nanhikali.org/pdf/TAG-Report.pdf
[21] Bed, Mattress, Chair, Table, Fan, Radio, TV (B/W and Colour), Pressure Cooker, Sewing Machine, Mobile Phone, Clock, Bicycle, and Water Pump
[22] Air Conditioner/cooler, refrigerator, motor bike, landline telephone, Internet, computer/laptop
[23] Authors’ calculation using NSSO data.
[24] See the section on Data and Empirical Strategy for a list of these items.
[25] Coefficients are not presented in Tables 2 and 3.
[26] Health is factored in, in the rights-based approach in terms of the quality of housing and access to services such as water and sanitation, childcare and other health services in order to make it adequate. The main thrust of the rights-based approach is on non- discrimination and equal access (UN 2018).



Find on this page
The Centre for Social and Economic Progress (CSEP) is an independent, public policy think tank with a mandate to conduct research and analysis on critical issues facing India and the world and help shape policies that advance sustainable growth and development.